


HER2+ advanced gastric cancer: Current state and opportunities (Review)
- Authors:
- Published online on: February 19, 2024 https://doi.org/10.3892/ijo.2024.5624
- Article Number: 36
-
Copyright: © Hu et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
1. Introduction
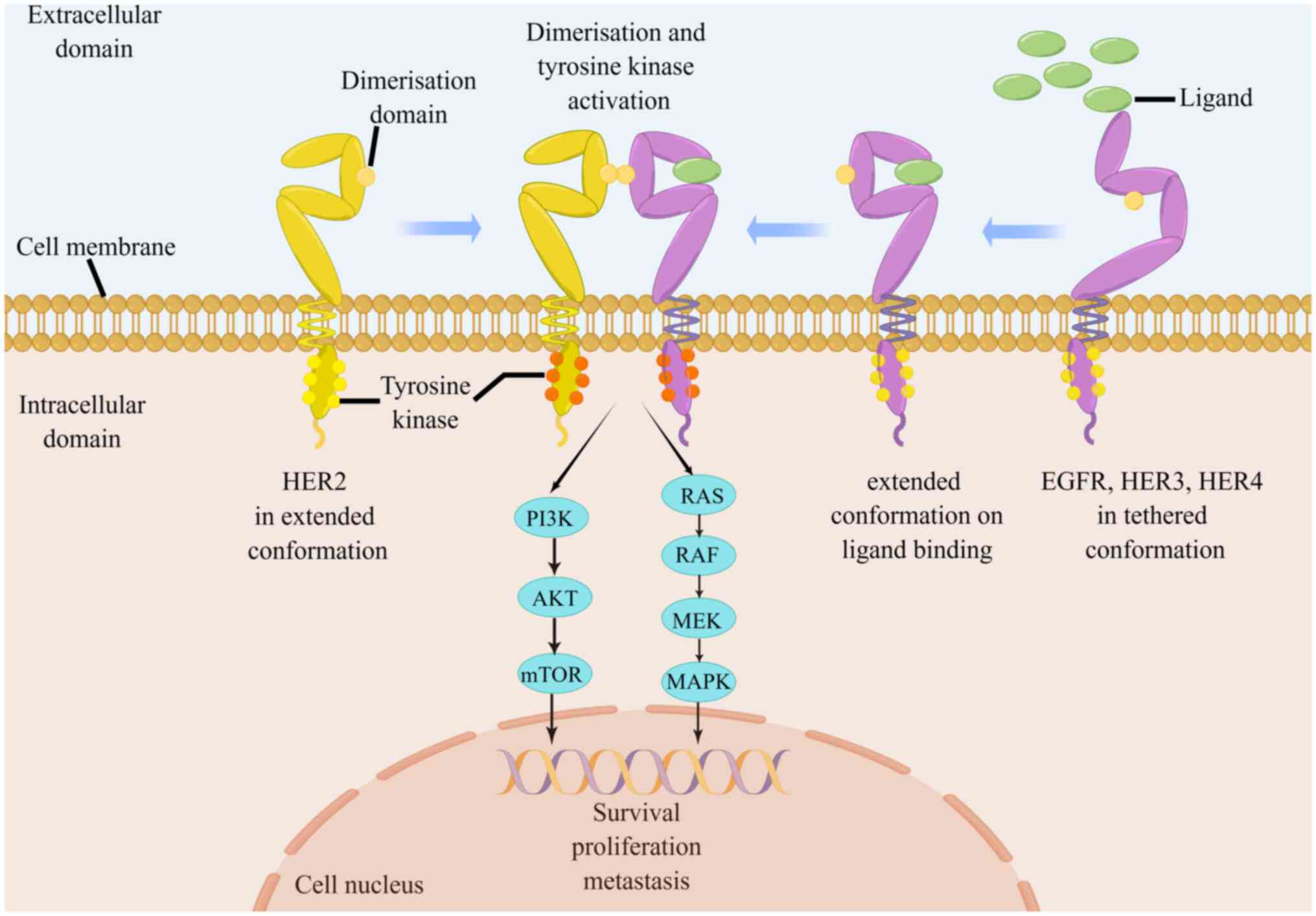
Gastric cancer (GC) is a prevalent malignancy with an incidence rate of 5.6% and a mortality rate of 7.7%, ranking 5th in incidence and 4th in mortality globally, adversely affecting the wellbeing and quality of life of patients (1,2). Human epidermal growth factor receptor 2 (HER2/ERBB2)+ GC is a key GC subtype, accounting for 10-20.2% of the total patients with GC (3). HER2+ GC refers to GC that is detected by immunohistochemistry (IHC) 3+ or IHC2+ simultaneous fluorescence in situ hybridization (FISH)+ according to the National Comprehensive Cancer Network guidelines (4). HER2, encoded by the oncogene ERBB2, is one of the most common and well-studied areas in advanced GC (AGC). HER2 protein forms heterodimers with other family members including EGFR, HER3, or HER4, which promote the autophosphorylation of intracellular tyrosine kinase domain to enhance HER2 activation. The phosphorylated tyrosine residues interact with several intracellular signaling molecules, leading to the activation of downstream pathways and cross-communication with other transmembrane signaling pathways, to regulate diverse biological effects (Fig. 1) (5-7). Overexpression of HER2 confers a heightened malignant phenotype to the tumor (5). Specifically, activated HER2 promotes GC cell proliferation and survival by regulating the expression of cycle-related proteins such as SKP2 and p27/Cdk2 (8-10). The overexpression of HER2 enhances vascular endothelial growth factor (VEGF) production and angiogenesis to accelerate tumor growth and metastasis (11,12). Furthermore, HER2 triggers epithelial-to-mesenchymal transition by activating the Wnt/β-catenin pathway. This activation, in turn, amplifies the migratory and invasive capabilities of GC cells (13,14). A thorough exploration of the features and underlying mechanisms of HER2+ AGC may reveal valuable insights for its effective management (15).
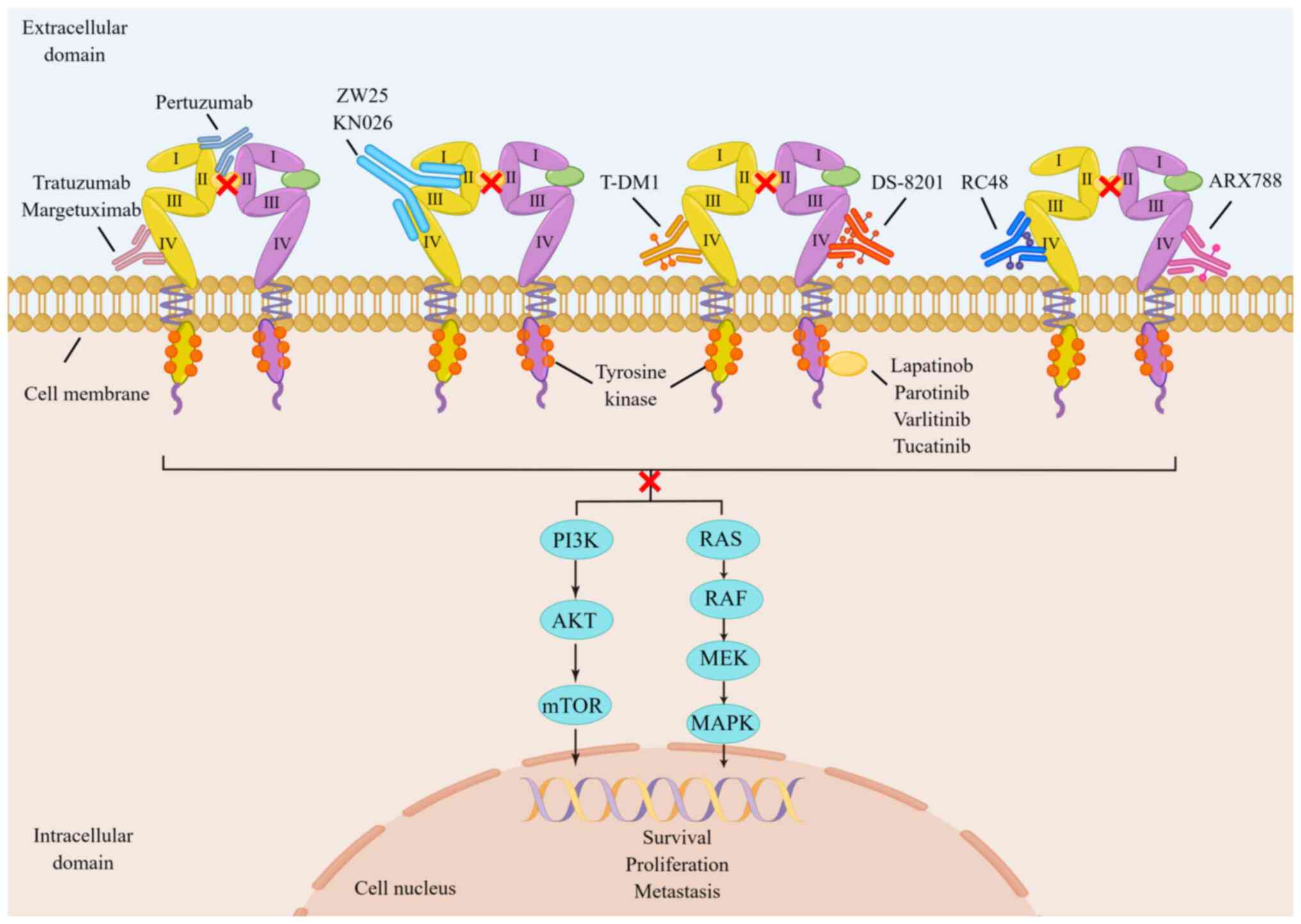
Numerous studies have demonstrated that targeted HER2 therapy can markedly improve the prognosis of patients with HER2+ AGC (16-18). Trastuzumab is a pivotal component of the initial anti-HER2-targeted therapy for HER2+ AGC, owing to its high efficacy (16). Currently, primary or secondary resistance to trastuzumab has been reported in most patients (17,19). Consequently, it is crucial to detect drug resistance and develop strategies to improve the sensitivity of patients to trastuzumab resistance. At present, aside from trastuzumab, DS-8201 and RC48 have also been approved for the posterior-line treatment of HER2+ AGC because of their notable efficacy in pre-clinical studies (20,21). A growing number of clinical and preclinical studies have also confirmed that anti-HER2-targeted drugs show good anti-tumor activity in HER2+ AGC (19-22). At present, anti-HER2-targeted drugs are available in four categories: Anti-HER2 monoclonal antibodies (McAbs), anti-drug conjugates (ADCs), bispecific antibodies and tyrosine kinase inhibitors (TKIs). They possess unique molecular structures and exert anti-HER2 targeting effects by acting on different targets of HER2 heterodimers (Fig. 2) (23-33). Additionally, several studies (34-36) have shown a trend to benefit the survival of patients with HER2+ AGC treated with immunotherapy drugs such as nivolumab and pembrolizumab in combination with targeted therapy (Table I). Through recent optimization and improvement, chimeric antigen receptor T-cell (CAR-T), a novel type of tumor precision targeted immunotherapy, has achieved good results in the treatment of clinical hematological tumors (37,38). It has also demonstrated good tolerance in preclinical studies in solid tumors, including AGC and has a wide range of exploration prospects (39,40). By analyzing and summarizing the preclinical and clinical studies of HER2+ AGC, the aim of the present review was to identify more effective therapeutic strategies for patients with this condition.
2. Current status and development of first-line treatment for HER2+ GC
Application and efficacy monitoring of targeted therapy
The ToGA study established trastuzumab as the first-line treatment of HER2+ AGC in 2010 (16). In that phase III clinical study, 594 patients with AGC and overexpression of HER2 from 24 different countries and regions were treated with either trastuzumab combined with chemotherapy (capecitabine or 5-Fu combined with cisplatin) or chemotherapy alone at a 1:1 ratio. Compared with the chemotherapy alone group, the former had significantly longer median overall survival (mOS; 13.8 vs. 11.1 months; P=0.0048) and median progression-free survival (mPFS; 6.7 vs. 5.5 months; P=0.0002), with the overall tumor response rate significantly improving (47 vs. 35%; P=0.0017). Nevertheless, there was no significant difference in toxicity curves between the two groups. At present, trastuzumab is the only anti-HER2-targeted drug approved for first-line treatment of HER2+ AGC in most countries around the world, including the United States, European Union countries, China, Japan and others.
Trastuzumab is frequently prescribed for patients with tumors and HER2 overexpression. Its effectiveness and duration are influenced by various factors, such as tumor cell evasion, diminished immune cell response and potential emergence of resistance at any stage of treatment (41-43). Timely monitoring and assessment of drug resistance status are advocated to optimize patient treatment plans and enhance treatment response rates in clinical practice. In 2018, Wang et al (45) found that the method of tumor tissue biopsy IHC/FISH was consistent (91.07%) with the detection of HER2 expression by plasma circulating tumor DNA (ctDNA). A further indication of the potential value of liquid biopsy in clinical practice is the fact that the change in the copy number of the HER2 in ctDNA can effectively feedback the efficacy of trastuzumab, and it is more sensitive than other markers like carcinoembryonic antigen and carbohydrate antigen 199 in predicting tumor size and progression. In another study (44), a Chinese team not only reached the same conclusions as Wang et al (45), but also discovered that in patients with acquired drug resistance, the level of HER2 somatic copy number alterations (SCNA) decreased. By contrast, the majority of patients with congenital trastuzumab resistance maintained high levels of HER2 SCNA in the progressive stage. Additionally, the authors found that PIK3CA mutations were enriched in patients with congenital drug resistance, with HER2/4 gene mutations being the most common, accounting for 35.3% (n=6) and 29.4% (n=5) of trastuzumab resistance in baseline and progression plasma, respectively (45). Patients with PIK3CA/R1/C3 or HER2/4 mutations had notably lower PFS in baseline plasma. Moreover, the study also confirmed that neurofibromatosis type 1 gene mutation can result in trastuzumab resistance. Trastuzumab resistance genes in HER2+ AGC should be monitored in clinical practice using the longitudinal ctDNA sequencing technique.
Recent studies have indicated that targeting the circadian rhythm may be a potential approach for treating HER2+ AGC (46,47). Time-based therapy involving metformin has been found to disrupt the BMAL1-CLOCK-PER1-HK2 axis and influence glycolytic oscillations, providing a means for alleviating trastuzumab resistance in HER2+ AGC (46). Moreover, another investigation using metabolomic analysis showed that patients with the GC T1 subtype (HER2+/MIB+/CD3+) had greater advantages from trastuzumab treatment compared with other subtypes (48). Effectively identifying specific subtypes is also considered a viable strategy for enhancing the specificity of trastuzumab treatment.
Exploration and efficacy of immunotherapy
The field of cancer treatment has been markedly transformed by immunotherapy, which is at present an integral component in the treatment of advanced cancer (49-51). Tumors may evade tumor immune monitoring and inhibit antitumor immune response through several mechanisms during the development and progression of cancer. Most of these mechanisms are associated with the participation of the immune checkpoint pathway. Anti-programmed cell death-1 (PD-1), which is expressed on the surface of T cells, is one of the innate immune checkpoints and important immunosuppressive transmembrane proteins. However, PD-1 on the surface of immune T cells will bind to PD-L1 abnormally expressed on the surface of tumor cells, inhibiting the killing effect of the immune system on tumor cells in the periphery (52,53). Immune checkpoint inhibitors (ICIs) are essential in activating the tumor immune response and restoring the monitoring function of immune T cells to tumor cells (54,55). It has been reported that HER-2-targeted therapy upregulates the expression of PD-1, cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) and tumour-associated macrophages (TAMs) within the tumor microenvironment, enhances the antibody-dependent cell-mediated cytotoxicity (ADCC) process, and improves the efficacy of immune therapy (56,57). Moreover, ICIs can reduce resistance to HER-2-targeted therapy (57,58).
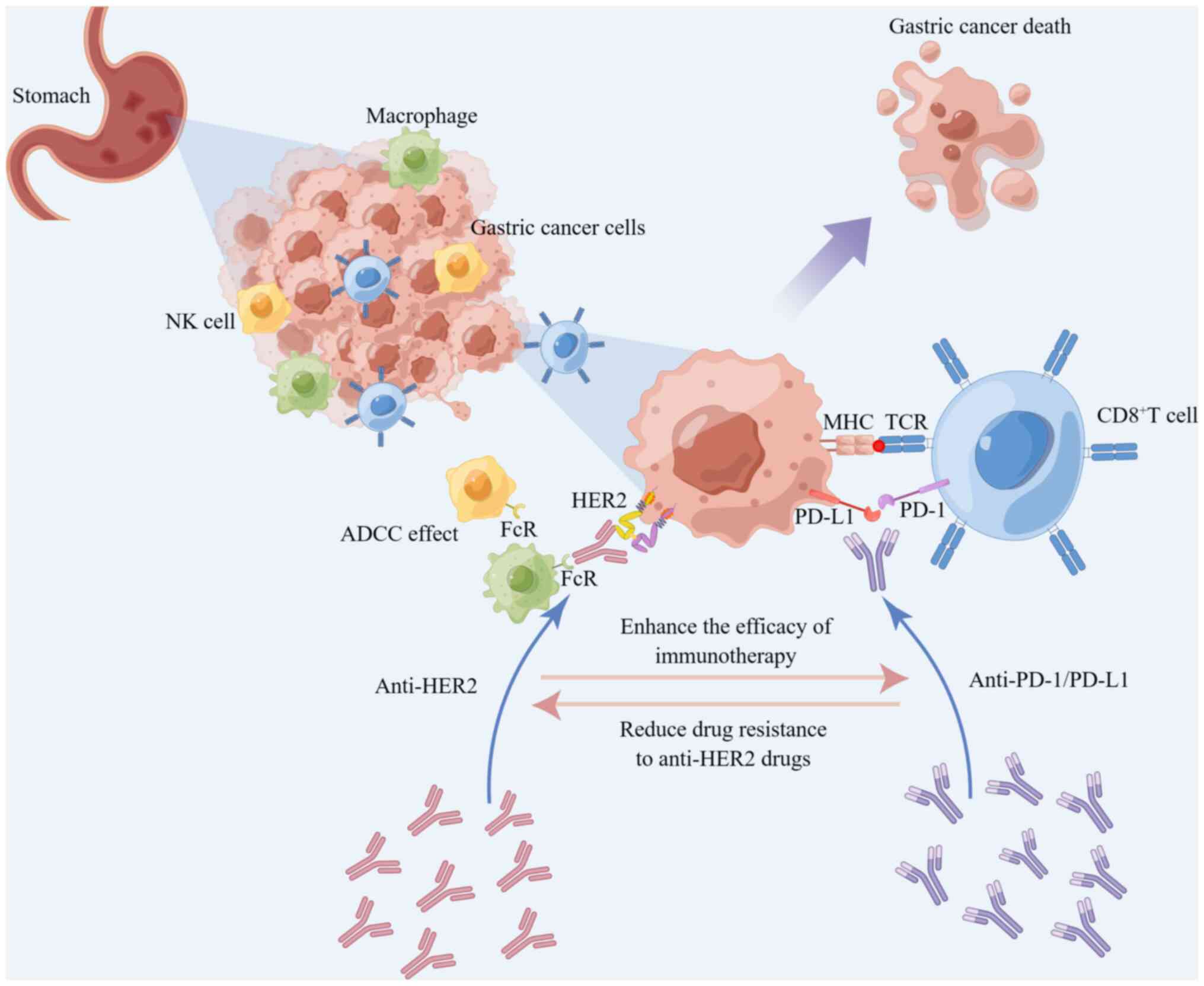
Numerous studies have demonstrated that adding PD-1/PD-L1 inhibitors to the standard treatment regimen of HER2+ AGC markedly improves the efficacy and survival time of patients (59-61). Combining the administration of ICIs with trastuzumab not only enhances the HER2-specific T-cell response, but also induces the transfer of immune cells to targeted sites, promoting the transformation and expansion of peripheral memory T cells (36,62,63). Trastuzumab upregulates the expression of PD-1 and PD-L1 as well as triggers the expression of tumor-infiltrating lymphocytes (52). Based on preclinical and clinical data, trastuzumab increased HER2 internalization and cross-presentation of dendritic cells, which further stimulated HER2-specific T-cell response, suggesting HER2 and PD-1 dual inhibition to potentially have a synergistic effect (Fig. 3) (35,64,65). Consequently, the combination of HER2 inhibitors with PD-1/PD-L1 inhibitors may synergistically suppress tumor cell survival, bolstering tumor-specific T cell immune responses. This strategy has the potential to enhance antitumor efficacy and increase the susceptibility of the tumor to clearance by the immune system.
To assess the preliminary efficacy of trastuzumab combined with pembrolizumab (a PD-1 inhibitor) and chemotherapy as first-line treatment, the PANTHERA trial (NCT02901301) enrolled a total of 43 patients with HER2+ AGC (three in phase Ib and 40 in phase II) for exploration. The result revealed that trastuzumab and pembrolizumab in combination with chemotherapy (cisplatin and capecitabine) had reliable safety and promising efficacy for treating HER2+ AGC regardless of the high expression of PD-L1. The results showed effective disease remission [overall response rate (ORR), 76.7%; disease control rate (DCR), 97.7%] and encouraging survival benefits [mOS, 19.3 months (95% CI, 16.5-NA) and mPFS ≤8.6 months (95% CI, 7.2-16.4)] (59). The combination of pembrolizumab, trastuzumab and chemotherapy may also exhibit potential activity in patients with HER2+ advanced gastroesophageal junction (GEJ) cancer according to a phase II trial (NCT02954536) (60). This is further confirmed by interim findings of the phase III KEYNOTE811 trial (NCT03615326) (35). The results demonstrated that the combination of pembrolizumab with trastuzumab and chemotherapy had a positive response as opposed to placebo as first-line therapy for HER2+ advanced GC and GEJ cancer (61). The complete response (CR) was notably improved (11 vs. 3%), and the ORR of pembrolizumab plus trastuzumab and chemotherapy reached 74.4; 22.7% higher than that of the placebo plus trastuzumab and chemotherapy group. Given the aforementioned results, in May 2021, the US Food and Drug Administration (FDA) approved pembrolizumab in combination with trastuzumab and chemotherapy as a first-line therapy for HER2+ AGC. This made pembrolizumab the first and only PD-1 inhibitor for first-line treatment of this GC type. A new treatment option for AGC is targeted therapy combined with immunotherapy.
Aside from pembrolizumab, other PD-1 inhibitors like nivolumab, tislelizumab as well as other ICIs including PD-L1 inhibitor avelumab and the CTLA-4 inhibitor ipilimumab, are being investigated as first-line drugs for HER2+ GC treatment. The combination of trastuzumab and anti-PD-1 antibody has been shown to increase the activity of trastuzumab-induced ADCC and demonstrate higher tumor regression in a preclinical investigation of HER2+ breast cancer (65). Nivolumab combined with trastuzumab and chemotherapy had reliable safety and good tolerance in patients with HER2+ AGC (UMIN000034222) according to the preliminary results of the Ni-HIGH study (66). Furthermore, the extended section of that study revealed that the combination regimen had good early efficacy in patients with HER2+ AGC. The ORR was 76.2% (95% CI, 60.6-86.9; CR, 4.8%; PR, 71.4%), and the DCR was 97.6% (67). A chemotherapy-free regimen, trastuzumab coupled with nivolumab and ipilimumab is also being tested to provide a novel treatment regimen for patients with HER2+ GC (NCT03409848) (68). Additionally, the ORR increased from 47 to 65% in a phase II study evaluating the efficacy of the combination of avelumab and trastuzumab with folinic acid, fluorouracil and oxaliplatin (FOLFOX) chemotherapy in previously untreated advanced GC/GEJ cancer, indicating that this combination therapy can benefit patients to some extent (69).
3. Research progress of second-line and posterior-line therapy
Prospect of trastuzumab after resistance to first-line therapy
The WJOG71112G (T-ACT) trial revealed that the effectiveness of continued use of trastuzumab as second-line therapy after disease progression on trastuzumab-based first-line therapy for HER2+ AGC is limited (70). Patients were randomly and equally assigned to paclitaxel and paclitaxel plus trastuzumab (PT) groups. The results showed that there was no survival benefit for patients in the experimental group compared with those in the paclitaxel group. The mPFS was 3.2 and 3.7 months, the mOS was 10 and 10 months and the ORR was 32 and 33% in the paclitaxel group and the PT group, respectively. These differences were not statistically significant, indicating that the continued use of the trastuzumab strategy in the posterior line did not significantly benefit patients with HER2+ AGC/GEJ cancer (70). However, a phase II clinical trial has revealed that the combination therapy of trastuzumab with ramucirumab, a VEGFR2 monoclonal antibody, and paclitaxel demonstrated considerable efficacy in patients previously treated for HER2+ GC/GEJ cancer. The mPFS and mOS were reported at 7.1 and 13.6 months, respectively, alongside a manageable safety profile (71). Targeting HER2 concurrently with the inhibition of VEGFR2 overexpression appears to exert a synergistic suppressive effect, potentially enhancing the sensitivity of patients with HER2+ AGC to trastuzumab.
An anti-HER2-targeted agent for second-line treatment, DS-8201
Trastuzumab, cleavable tetrapeptide junction, and cytotoxic topoisomerase I inhibitor (camptothecin derivative DXd) are the active ingredients in DS-8201, a second-generation ADC drug (23). DS-8201 has more advantageous drug payload and higher drug antibody ratio (8 vs. 3.4) than T-DM1. While T-DM1 degrades when it enters tumor cells, DS-8201 has a better junction that is stable in plasma and spread across the membrane to neighboring tumor cells to play the cytotoxic bystander effect and lower the dependence of DS-8201 treatment on HER2 expression (23,72). These advantages make DS-8201 preferable in the AGC treatment with notable HER2 expression heterogeneity. DS-8201 showed good antitumor activity in patients with AGC patients and high as well as low HER2 expression in some phase I clinical studies (73,74). The response rate of patients treated with DS-8201 for severe preconditioning HER2+ AGC was ~40%, indicating good antitumor activity and safety. Moreover, the phase II DESTINY-Gastric01 study (20) compared the therapeutic efficacy of DS-8201 with standard chemotherapy in patients with HER2+ AGC/GEJ cancer who had received ≥2 types of treatment, including trastuzumab. The treatment with DS-8201 markedly improved the ORR of patients (51.3 vs. 14.3%) and mOS (12.5 vs. 8.4 months) compared with standard chemotherapy. These findings led to the approval of DS-8201 for the treatment of patients with AGC/GEJ cancer who had previously undergone first-line therapy that included trastuzumab. Hence, DS-8201 is the first anti-HER2-targeted ADC drug for second-line treatment of HER2+ AGC.
An anti-HER2-targeted agent for third-line treatment, RC48
RC48 is composed of hertuzumab with improved affinity and endocytosis, a cleavable linker and a cytotoxic drug monomethyl auristatin E (MMAE). Its increased applicability to patients with low expression tumor HER2 is due to its ability to exert a similar bypass killing effect as DS-8201 (24,75). A phase I study (76) revealed that RC48 had good tolerability and effective antitumor activity in various HER2+ solid tumors, including AGC in HER2 IHC2+/FISH− state. The ORR, DCR, mPFS and mOS of patients with HER2+ AGC (including HER2 IHC2+/FISH− status) who had received ≥2 types of systematic chemotherapy was 24.4, 41.7%, 4.1 months and 7.6 months, respectively, after receiving RC48 treatment, according to a single-arm multicenter phase II trial (21). These findings suggest that RC48 is a possible third-line therapeutic option for patients with HER2+ AGC, and has good efficacy and great potential. Based on that study, National Medical Products Administration approved RC48 as a third-line targeted therapy of patients with HER2+ AGC/GEJ cancer who had received ≥2 types of systematic chemotherapy, filling the gap for HER2+ AGC. In addition, RC48 in combination with immune checkpoint PD-1 inhibitors (pembrolizumab or atezolizumab) showed good efficacy (36) in mice, and induced lasting immune protection in a HER2+ breast cancer mouse model. This could be due to the increase of T-cell infiltration in the tumor caused by MMAE, a toxin molecule present in RC48. The combination regimen may aid in resolving drug resistance problems in some patients with AGC after treatment with RC48.
Research progress in other posterior line therapies
At present, there are no other HER2-targeted medications licensed for use in posterior-line therapy, with the exception of DS8201 and RC48, which are approved for use in the second and third lines of treatment of HER2+ AGC. As a second-line treatment for HER2+ AGC, the phase III GATSBY study examined the safety and effectiveness of the T-DM1 (ADC) in conjunction with paclitaxel compared with paclitaxel alone; no notable results were observed (77). In a phase II trial, patients with HER2+ AGC who had ≥1 prior round of conventional treatment showed marked and long-lasting remission (ORR, 56%; 95% CI, 35-76%) from the bispecific antibody KN026 (78). In addition, the results of the phase I clinical trial on another bispecific antibody, ZW25, suggest potential advantages for third- or fourth-line treatment in HER2+ patients with AGC. These findings provide encouragement for further clinical research into ZW25 and other drug combination therapies for patients with HER2+ AGC (79).
When immunotherapy was initially used as a third-line treatment for AGC, it showed considerable success. The phase II KEYNOTE-059 study (NCT0233511) shown that the study population, which included patients with HER2+ or HER2− AGC and had previously received trastuzumab treatment, could benefit from it independently of their PD-L1 status (80). However, later phase II/III KEYNOTE-061 trial investigations indicated that compared with paclitaxel, pembrolizumab monotherapy did not markedly enhance OS in patients with AGC (81). The CP-MGAH22-05 study demonstrated a synergistic antitumor effect when combining pembrolizumab, an anti-PD-1 checkpoint inhibitor, with margetuximab, a fragment crystallizable (Fc) optimized anti-HER2 drug. Among the 92 evaluable patients with HER2+ AGC who had previously received ≥1 conventional trastuzumab-containing therapy, a favorable ORR was observed in 17 patients (18.48%; 95% CI, 11.15-27.93) (82). Consequently, the combination regimens of ICIs and anti-HER2-targeted drugs may become a promising option for post-treatment of patients with HER2+ AGC and trastuzumab resistance.
4. Research progress of other potential anti-HER2-targeted drugs
Anti-HER2 McAbs
Pertuzumab is a recombinant human McAb that primarily disrupts the dimerization of HER2 and other family members to play a targeted role different from the binding site of trastuzumab (25). The combination of pertuzumab and trastuzumab has a stronger inhibitory effect on HER2 overexpression, as well as better therapeutic effect than trastuzumab alone. This dual-targeted therapy markedly improves colorectal cancer treatment outcomes and prolongs the survival of patients of breast cancer for 10 months (83). Pertuzumab combined with trastuzumab had greater antitumor activity than single-targeted therapy in the xenotransplantation model of HER2+ AGC (84). The JACOB phase III clinical trial (85) examined the effectiveness of pertuzumab in combination with trastuzumab and chemotherapy in patients with HER2+ metastatic GC/GEJ cancer. Although there were no statistically significant results in terms of the OS between the pertuzumab group and the control group, the pertuzumab group showed a 3.3-month increase in the mOS compared with that in the control group (17.5 vs. 14.2 months; HR, 0.84; 95% CI, 0.71-1.00; P=0.057). According to the Chinese subgroup analysis, the mOS for the pertuzumab group and control group was 18.7 and 16.1 months (HR, 0.75; 95% CI, 0.49-1.14), respectively, and the mPFS was 10.5 and 8.6 months (HR, 0.85; 95% CI, 0.60-1.21), respectively (86). The therapeutic effect of the Chinese population (86) was comparable with that of the global intention-to-treat analysis population, with the HR of the mOS and the mPFS being lower than those of the control group. Pertuzumab combination with trastuzumab and chemotherapy as a first-line treatment could prolong the survival time of Chinese patients with HER2+ AGC. Furthermore, the treatment regimen was well-tolerated in the patients. Pertuzumab plus trastuzumab and chemotherapy also increased the ORR of the perioperative patients with HER2+ AGC from 25 to 45% according to the INNOVATION trial (87). Tumor heterogeneity and population differences affect the efficacy of trastuzumab combined with pertuzumab. Therefore, it is necessary to further improve the trial design and selection criteria to identify patients who are more likely to benefit from dual anti-HER2-targeted therapy.
Margetuximab and trastuzumab have similar HER2 binding as well as antitumor proliferation effects. Compared with trastuzumab, margetuximab has greater antitumor activity in vitro due to its improved Fc domain, which also improves immunological mechanisms such as ADCC (26,88). A phase I study (89), showed that margetuximab has good tolerance and antitumor effectiveness when used as a monotherapy against a variety of solid tumors with HER2 overexpression, including AGC. After the successful III phase SOPHIA trial, FDA approved margetuximab in combination with chemotherapy as the first-line treatment for previously treated metastatic HER2+ breast cancer (90). Catenacci et al (82,91-94) conducted multiple preliminary studies on the efficacy of combining margetuximab and pembrolizumab in treating HER2+ AGC. One of these studies (82), CP-MGAH22-05, is a single-arm, phase IB/II trial to evaluate the safety and tolerance of margetuximab combined with pembrolizumab in the treatment of patients with HER2+ GEJ cancer. There was no statistically significant dose-limiting toxicity in the dose-increasing phase, with the combined therapy having acceptable safety and tolerance. Furthermore, the phase II/III MAHOGANY clinical trial (95), currently being conducted by Catenacci et al is an exploratory attempt to integrate margetuximab with other new immunotherapeutic drugs including retifanlimab and tebotelimab as a novel method for HER2+ AGC treatment. Previous studies suggest that double inhibition of PD-1 and lymphocyte-activation gene 3 (LAG-3) targeting could enhance the efficacy of margetuximab by strengthening the innate and adaptive immune response to tumor cells overexpressing HER2 (96-98). According to researchers, targeting HER2 and PD-1 using margetuximab plus retifanlimab, or HER2 and PD-1 plus LAG-3 by combining margetuximab plus tebotelimab presents a chance to augment antineoplastic response in patients with HER2+ AGC compared with single drug treatment.
ADCs
The combination of trastuzumab and mitotic inhibitor emtansine forms a complex T-DM1 (29). Numerous pivotal phase III studies have shown that T-DM1 markedly prolonged the OS and PFS of patients with metastatic HER2+ breast cancer compared with traditional chemotherapy (99-101). By contrast, the multicenter randomized controlled phase II/III Gatsby study (77) revealed that patients with HER2+ AGC treated with T-DM1 lacked survival advantages compared with those treated with paclitaxel or docetaxel. Patients who received T-DM1 had a mOS of 7.9 months, whereas those who received taxane had a mOS of 8.6 months. There was no statistically significant difference between the two treatment groups (HR, 1.15; 95% CI, 0.87-1.51; P=0.86). These findings suggest that T-DM1 may not have an additional therapeutic advantage in this patient population. This could be because AGC has notable heterogeneity, and some patients have hereditary or acquired drug resistance to T-DM1. A study demonstrated that the upregulation of recombinant matrix metalloproteinase 7 (MMP7) has a strong relationship with the drug resistance of AGC cells to T-DM1 (102). The activation of MMP7 during this process has been found to be influenced by DKK1 and Wnt/β-catenin.
A humanized McAb that specifically targets the HER2 protein on cancer cells and a cytotoxic tubulin inhibitor known as AS269 that is conjugated to the McAb const ARX788, a site-specific anti-HER2 antibody-drug combination (30,103) In preclinical studies, ARX788 demonstrated effective anticancer activity in breast cancer and AGC with minimal expression of HER2 and T-DM1 resistance in addition to good safety and antitumor activity in AGC and breast cancer with overexpression of HER2 (104,105). The results of a multicenter dose-expanded phase I clinical trial (106) showed that ARX788 had good tolerance and antitumor efficacy in patients with HER2+ AGC/GEJ cancer who were non-responsive to trastuzumab. The patients had an ORR of 37.9% and a DCR of 55.2%. With a median follow-up of 10 months, the mPFS and mOS were 4.1 and 10.7 months, respectively (CTR20190639). At present, other clinical trials of ARX788 for AGC treatment are ongoing (NCT03255070 and CTR20201708).
Bispecific antibodies
ZW25 is an example of a HER2-targeted bispecific antibody, which can simultaneously bind two non-overlapping epitopes of HER2, the trastuzumab-binding domain ECD4 and the pertuzumab-binding domain ECD2 (27). Preclinical studies (107,108) have indicated that ZW25 exhibits good antitumor activity and can silence HER2 signaling in xenograft mouse models expressing HER2, including GC. Meric-Bernstam et al (109) confirmed the safety and efficacy of ZW25 in patients with advanced solid tumors expressing HER2 in this phase I study. A phase I basket trial (108) showed that patients, including 10 patients with GEJ cancer, five patients with colorectal cancer and nine patients with other malignant tumors except breast cancer, treated with ZW25 had a high ORR (41%) with mild side effects most of which were rated as grade 1 or 2. At the network meeting of the American Society of Clinical Oncology-Gastrointestinal Cancers Symposium (ASCO-GI) in 2021, the phase I clinical trial (79) of ZW25 on third-line and fourth-line treatment of patients with HER2+ AGC showed that ORR and DCR of ZW25 monotherapy were 33 and 61% respectively, while the combined chemotherapy showed better efficacy, with ORR of 54% and DCR of 79% (NCT02892123). This result revealed the great potential of ZW25 as a posterior line therapy. The safety and antitumor efficacy of ZW25 in combination with other drugs for the treatment of HER2+ AGC (NCT04276493, NCT03929666 and NCT05027139) is currently being investigated in several phase I and II clinical trials.
KN026 can target two non-overlapping epitopes on HER2 derived from trastuzumab (domain IV) and pertuzumab (domain II) simultaneously, to achieve the combination effect of trastuzumab and pertuzumab (110). In addition, KN026 had an inhibitory effect on some tumor cells with low HER2 expression and trastuzumab-resistant cell lines (78,110). The safety and pharmacokinetics of KN026 as a monotherapy, even in patients with more severe preconditioning was recently evaluated in a first phase I study in patients with HER2+ metastatic breast cancer (111). That study showed that patients who benefit more from treatment with KN026 may be defined by co-amplification of HER2/CDK12. Additionally, KN026 has demonstrated promising efficacy as an initial treatment for patients with AGC/GEJ cancer with HER2 expression (112). The findings of an ongoing phase II study on KN026, which was presented at the ASCO-GI annual meeting in 2021, indicated that KN026 is effective in treating HER2+ AGC/GEJ cancer, regardless of prior treatment with trastuzumab. According to the study, the ORR was 55.6% and the DCR was 72.2% in patients with high HER2 expression. The ORR and the DCR in patients who previously received trastuzumab were 44.4 and 66.7%, respectively. A phase II study of KN026 was conducted on patients with HER2+ AGC who had undergone ≥1 round of standard chemotherapy. That study indicated an ORR of 56% for the HER2 overexpression group with an acceptable safety (NCT03925974) (78). There are several phase I/II clinical trials (NCT03925974; NCT03619681; NCT03847168) ongoing. The CDE has officially approved the phase III clinical trial application of KN026 combined with chemotherapy for AGC/GEJ with disease progression after receiving standard first-line chemotherapy, implying that KN026 has the potential as a HER2-targeted drug. Additionally, several studies have demonstrated that KN026 combined with anti-PD-L1/CTLA-4 bispecific antibody KN046 has favorable safety, tolerability and efficacy in patients with HER2+ gastrointestinal tumors as well as other HER2-abnormal solid tumors (113-115). Therefore, combining KN026 with other targeted drugs may provide a better treatment option for patients with HER2+ AGC.
IBI315 is the first anti-HER2/PD-1 bispecific antibody in the world. It can simultaneously bind PD-1 molecules on T cells and HER2 molecules on tumor cells, and act as an immune activator and tumor cell inhibitor. The remarkable therapeutic effects of IBI315 were observed in preclinical models, including organoids. Furthermore, IBI315 demonstrated the capacity to regulate gasdermin B expression in tumor cells, specifically in HER2+ AGC, inducing cell pyroptosis and promoting T cell activation. Activated T cells release IFNγ, further enhancing gasdermin B expression, creating a positive feedback loop that efficiently eradicates HER2+ GC cells (116). CIBI315A101 is the first clinical trial (NCT04162327) to assess the safety, tolerance and efficacy of IBI315 monotherapy and combination chemotherapy for patients with advanced solid malignant tumors expressing HER2. The preliminary results of dose escalation of this trial presented orally at the Chinese Society of Clinical Oncology in 2021 demonstrated good safety and efficacy.
TKIs
Lapatinib, a small molecule oral drug, is a dual EGFR/HER2 TKI (31). The phase III TRIO-013/LOGIC randomized trial assessed the effectiveness of lapatinib in the initial treatment of HER2+ AGC. Results showed that that the addition of lapatinib to CapeOx did not markedly improve the OS of patients (117), but pre-planned exploratory subgroup analysis showed that OS was prolonged in the lapatinib group for Asian and young patients (<60 years old). A similar study confirmed that the PFS of Asians and patients <60 years old was markedly improved among patients treated with lapatinib, and the benefit was more notable in patients with >5-fold increase in HER2 expression (118). In the second-line treatment of patients with AGC and HER2 overexpression, the phase III TyTan trial demonstrated that compared with paclitaxel monotherapy, lapatinib combined with paclitaxel exhibited higher efficacy in the Asian population. However, this regimen did not markedly improve the OS of patients (119). Consequently, this study did not validate the reported increase in OS among Asian patients undergoing lapatinib treatment as indicated in the TRIO-013/LOGIC study (31,119). Previous studies have shown that MET and CCNE1 amplification contribute to the occurrence of lapatinib resistance (97). Recent studies have also found that (120,121) loss of function mutations in CSK and PTEN promoted lapatinib resistance by reactivating the MAPK and PI3K pathways. Further in vitro and in vivo trials demonstrated that synergistic inhibition of these two pathways effectively overcame the drug resistance against Lapatinib induced by HER2 amplification in AGC (120,121).
Pyrotinib is a novel pan-HER small molecule TKI which irreversibly binds to the ATP binding sites of HER1, HER2 and HER4 intracellular kinases (32). Consequently, it blocks the activation of downstream signal pathways, thereby inhibiting the growth of tumor cells (122,123). Some studies have shown that pyrotinib can effectively treat HER2+ advanced solid tumors (124,125) without notable toxicity. Additionally, the combination of pyrotinib and SHR6390, a CDK4/6 inhibitor, showed good efficacy and safety in treating patients with refractory HER2+ AGC and solid tumors (126). In one case report (127), a 72-year-old male patient with HER2+ AGC developed resistance to trastuzumab and camrelizumab (a PD-1 inhibitor) combined with apatinib. When the patient was treated with capecitabine combined with pyrotinib, the tumor size was markedly reduced, which prolonged the patient's survival. The patient has survived for >30 months after postoperative recurrence and is currently receiving combination therapy with pyrotinib and capecitabine, with a PFS >8.5 months. Furthermore, several analogous cases have shown a favorable outcome following pyrotinib administration as a later-line treatment (128-130). Pyrotinib may be another promising targeted drug for the treatment of HER2+ AGC.
Varlitinib is a reversible pan-HER TKI. In a patient-derived xenograft model of GC expressing HER2, it was found that varlitinib induced antitumor activity (33). A phase II trial of varlitinib as the first-line treatment of patients with AGC co-expressing HER1/HER2 (NCT03130790) showed that varlitinib did not reach the primary endpoint of marked tumor size reduction after 12 weeks of treatment. Another phase IB clinical trial (KCT0003583) for varlitinib in combination with paclitaxel as a second-line therapy for HER1/HER2 co-expressing AGC indicated that the combination treatment had a favorable safety profile (131). Currently, the multi-site phase II clinical trial are under way (KCT0003583) to test the efficacy of this treatment (131).
Tucatinib, a highly selective small molecule HER2-targeted TKI, has been shown to markedly improve the OS of patients with breast cancer (132). Additionally, it is currently being investigated as a potential treatment for advanced colorectal cancer and other gastrointestinal tumors, including AGC. In GC/GEJ cancer xenotransplantation models, dual targeting HER2 of tucatinib and trastuzumab showed superior antitumor activity compared with any single drug treatment (133). These data support the clinical application potential of tucatinib. The mid-term results of MOUNTAINEER trial (NCT03043313) showed that tucatinib and trastuzumab had marked antitumor activity in HER2+ colorectal cancer (134). The MOUNTAINEER-02 trial, a phase II/III study (NCT04499924), is currently been conducted (135,136) to evaluate the effectiveness of tucatinib, ramucirumab, and paclitaxel in treating HER2+ AGC/GEJ cancer. The trial aims to determine the effectiveness of tucatinib compared with that of ramucirumab and paclitaxel as single drug treatments for this type of cancer.
5. New methods for the treatment of HER2+ AGC
CAR-T cell therapy
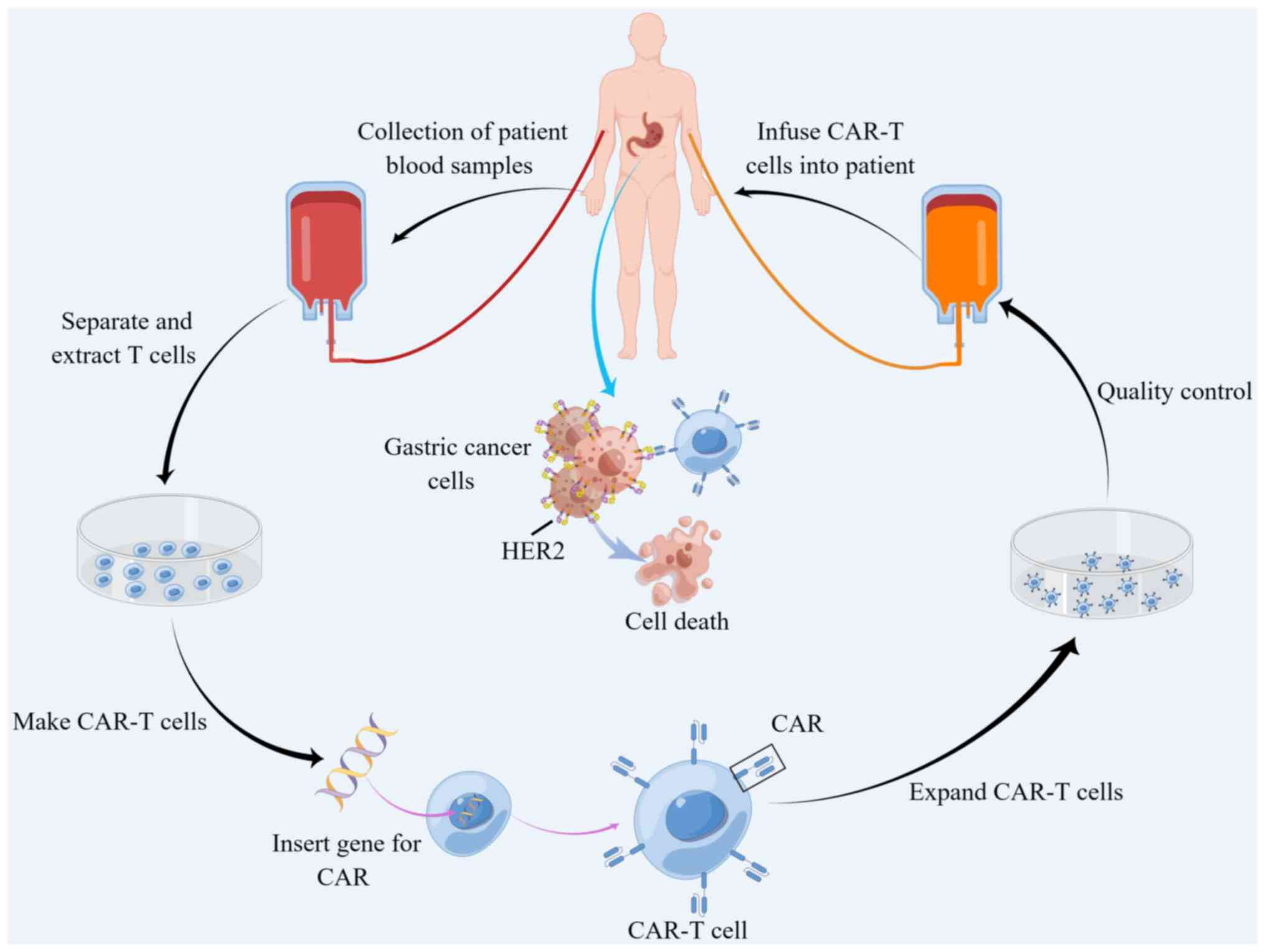
CAR-T cell therapy is an innovative technique for treating cancer that involves genetic engineering of T lymphocytes removed from patients, with the goal of directing them towards cancer cells (137,138). Initially, CAR-T cell therapy was used to treat hematological malignancies with satisfactory outcomes (139,140). Therefore, it has become the preferred therapy for patients showing resistance to conventional chemotherapy or radiotherapy (141). In recent years, studies found that CAR-T elicit good response from various solid tumors (39,142). HER-2-targeting CAR-T cells for AGC are currently been investigated to develop strategies to reduce drug resistance and improve therapeutic effect (Fig. 4) (143). In another study, a novel type of genetically modified human CAR-T cells targeting the GC cell antigen HER2 was developed. These cells embody the CD137 and CD3ζ moieties (40). The activated CAR-T cells, expanded in number, effectively target HER2 antigens in an major histocompatibility complex-independent manner, and demonstrate notable efficacy in eliminating HER2+ GC cells derived from patients. Furthermore, CAR-T cells exhibited markedly enhanced tumor inhibition and targeting in HER2+ xenograft tumors compared with controls (40). A preclinical study (144) reported that humanized chimeric antigen 21 (ChA21) single chain antibody fragment-based CAR-T cell therapy can treat AGC with overexpression of HER2. The important constituent of this specific CAR-T cell, 4-1BBz, is constructed from the intracellular domain of 4-1BB (TNFRSF9 or CD137) and the CD3z signaling domain. ChA21-4-1BBz CAR-T cells showed specific helper T cell 1 skewed cytokine response and efficient cytolysis of human GC cells with high expression of HER2 in vitro, and its effect was mediated by HER2 expression on the surface of tumor cells. In the established models of subcutaneous xenotransplantation and peritoneal metastasis, chA21-4-1BBz CAR-T cells markedly promoted the regression of tumors with HER2 overexpression, prolonged the survival time of mice bearing HER2+ tumors, and enhanced the circulatory ability of CAR-T cells, as well as their specific fate and accumulation at the tumor site (144).
In terms of the clinical application of CAR-T in other solid tumors, there is a need to balance between its side effects and curative effects. A phase I clinical trial (NCT01935843) (145), evaluating the safety, feasibility and activity of HER2 immunotherapy for patients with advanced biliary tract cancer and pancreatic cancer, showed that 1/11 selected patients developed partial response (PR) for 4.5 months, and five patients were in stable disease (SD) and their mPFS was 4.8 months, indicating that the immunotherapy had good clinical efficacy. Nevertheless, two patients experienced severe upper gastrointestinal bleeding, suggesting a potential threat of HER2-targeted CART cells in anti-tumor process. The CAR-T cell therapy targeting other gastrointestinal cancer markers, such as claudin 18.2 and 6, has also shown promising efficacy in early clinical trials (146-148). Therefore, by optimizing the design of CAR-T cell therapy involving regulation of the tumor load, and antigen expression and distribution, its clinical application in patients with HER2+ AGC may be feasible.
HER2-targeted vaccines
Tumor vaccines have become research hotspots in recent years. Various forms of tumor antigens, such as tumor-related proteins, peptides and genes expressing tumor antigens have been introduced to patients to overcome immunosuppression caused by the tumors, enhance immunogenicity, stimulate the patient's immune system, and induce cellular and humoral immune responses to control or eradicate the tumors (149,150). At present, diverse vaccine types, including DNA, mRNA, polypeptides and dendritic cell vaccines have been formulated to stimulate the body's immune response against cancer cells. These vaccines are specifically designed based on the biological characteristics of HER2 expression in tumor cells (151,152). There have been marked developments in research on HER2-targeted vaccines and their application in the treatment of advanced breast cancer (152-155). This suggests that other solid tumors with similarly high HER2 expression may benefit from such therapies. A research team from Austria developed a therapeutic B cell epitope vaccine (IMU-131/HER-Vaxx), composed of three fused B cell epitopes from the HER2 extracellular domain coupled to CRM197 with Montanide as an adjuvant (156). The team further conducted a phase IB clinical trial (NCT02795988) and evaluated the immunogenicity and optimal dose (detection dose, 10, 30 or 50 μg) in patients with HER2+ AGC based on the HER2 specific antibody and cellular response. The results showed that none of the 11 patients experienced major adverse reactions, and one patient had a complete response, five patients had partial response, and four patients had stable disease, indicating that IMU-131 had good tolerability, safety and therapeutic potential (156). The induced HER2-specific antibody and cell response showed a dose-dependent relationship and it was markedly associated with clinical response. Therefore, the recommended maximum dose (50 μg) has been applied in phase II clinical trials to further evaluate clinical response.
6. Conclusion and prospects
Taken together, trastuzumab is still the first-line treatment for patients with HER2+ AGC targeting HER2. However, its efficacy is limited by the development of drug resistance. The expression of HER2 should be detected using ctDNA to monitor the efficacy of trastuzumab, and liquid biopsy may also help to predict tumor progression. In addition, anti-HER2-targeted therapy combined with immunotherapy has become a novel approach for improving the prognosis of patients with HER2+ AGC. Moreover, investigating new therapy strategies, such as therapy based on biological rhythms or identifying specific subtypes sensitive to HER2 targeting, would be an attractive strategy for increasing the efficacy of trastuzumab in the treatment of HER2+ AGC (46,48). Meanwhile, ADC drugs such as DS-8201 and RC48, have been approved as second-line and third-line treatments for patients with HER2+ AGC, respectively (20,21). Anti-HER2 bispecific antibodies such as MGAH22 and ZW25 have good efficacy. However, given their widespread use in the treatment of breast cancer, anti-HER2-TKIs have not been approved for GC treatment. This may be explained by the high heterogeneity of GC (157,158).
The advent of CAR-T cell therapy has revitalized prospects for patients with HER2+ AGC. While CAR-T cell therapy for solid tumors poses challenges distinct from hematological tumors, the approach of targeting various antigens through CAR-T cell therapy can still yield positive outcomes for specific patient groups. Simultaneously employing ICIs to counteract immunosuppressive factors within the tumor microenvironment holds promise for enhancing the effectiveness of CAR-T cells in HER2+ AGC (148,159,160). HER2-targeted cancer vaccines can activate the patient's own immune system to kill cancer cells, providing a more durable therapeutic effect. However, it is noteworthy that HER2 cancer vaccines are still in the early stages of development. Immunologic escape and immune tolerance remain major challenges that limit their progress (156,161). Further research is required to identify optimal conditions for their use and potential side effects. Moreover, there is a need to develop strategies to identify patients who may benefit from targeted therapy and immunotherapy, while also monitoring drug efficacy. This will lead to the development of novel drugs and strategies for the management of HER2+ AGC.
Availability of data and materials
Not applicable.
Authors' contributions
HHH was responsible for writing the majority of the manuscript and preparing the figures and tables. SQW revised the manuscript. HCZ and ZSC supervised the process and participated in writing the manuscript. XBC and XJS conceived the study and provided oversight throughout the process. All authors have read and approved the final version of the manuscript. Data authentication is not applicable.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Acknowledgments
Not applicable.
Funding
The authors would like to thank for the financial support provided by the National Natural Science Foundation of China (grant nos. 82103560 and 82103996), the Young and Middle-Aged Health Science and Technology Innovation Talent Training Project of Henan Province (grant nos. YXKC2022048 and YXKC2020008), the Science and Technique Foundation of Henan Province (grant no. 202102310413) and the Natural Science Foundation of Henan Province (grant nos. 232300421119, 212300410270 and 212300410253).









