



Effect of thickeners combined with swallowing exercises for patients with post‑stroke dysphagia
- Authors:
- Published online on: March 27, 2024 https://doi.org/10.3892/wasj.2024.239
- Article Number: 24
-
Copyright : © Pham et al. This is an open access article distributed under the terms of Creative Commons Attribution License [CC BY 4.0].
Abstract
Introduction
Stroke is a major global health concern and the second leading cause of disability and mortality worldwide (1). In Vietnam, stroke is the leading cause of mortality and disability (2). Dysphagia is defined as an impairment in swallowing that results in an abnormal transit of a liquid or solid bolus from the oral cavity to the stomach. The antero- or retrograde entry of saliva, food or gastric secretion into the airway under the level of the vocal folds is defined as aspiration. This is very common following a stroke, causing aspiration pneumonia with a prevalence of up to 80% (3). The early detection of problems with swallowing not only reduces the risk of pneumonia, but also helps to minimize the risk of malnutrition, dehydration, the length of hospital stays and mortality, and allows for the spontaneous recovery of swallowing functions. A number of treatment approaches for swallowing disorders have been proposed, including compensatory strategies, rehabilitation techniques, invasive interventions and surgical management. Swallowing rehabilitation is considered a safe and highly effective treatment method for patients to help prevent complications, thereby significantly reducing mortality (4).
The management of swallowing disorders consists of using thickeners to control and prevent aspiration pneumonia. During the oral phase of swallowing, the fluid flow is disturbed. A person can tolerate these factors, and the substances will pass through the airways into the esophagus. However, individuals with dysphagia may have trouble controlling this process, and this affects their ability to protect the airway. One of the solutions is to alter the consistency of the fluid with a thickener for improved swallowing coordination. Thickeners are safe and have been used therapeutically for swallowing disorders for the past 19 years. The European Society for Swallowing Disorders (ESSD) concluded that increasing the consistency reduces the risk of aspiration and is a valuable management strategy for dysphagia (5).
A number of studies have been conducted to examine the influence of bolus consistency on swallow safety and effectiveness. Kuhlemeier et al (6) examined 190 patients using videofluoroscopy (VFS; videofluoroscopic swallowing examination) with mild to moderate dysphagia due to several causes. The results of their study revealed that the prevalence of aspiration was higher when swallowing thin liquids with a cup than when swallowing ultrathick liquids with a spoon (6). In their study, xanthan gum was used as a thickener, and the results also revealed a significant reduction in the aspiration rate from 35.3 to 13.7% with the use of thin liquids with nectar consistency, and to 9.3% with the use of spoon-thick liquids (6). Clavé et al (7) reported that penetration into the laryngeal vestibule was the most common indicator of impaired swallow safety and occurred most frequently with liquid bolus (21.6 mPa.s), less with nectar (295.0 mPa.s), and least with pudding viscosity (3682.2 mPa.s). Diniz et al (8) conducted a study on 61 patients following a stroke by increasing the food consistency from thin to a spoon thick (very thick), and the results revealed a significant reduction in the aspiration rate. Rofes et al (9) reported that altering the bolus consistency from liquid to pudding reduced the prevalence of aspiration and pneumonia in 98.9% of patients.
According to the study by Jongprasitkul and Kitisomprayoonkul (10), conventional swallowing therapy including swallowing exercises and maneuvers, postural and compensation techniques, food and environmental modification, and alternative feeding was an effective treatment for patients with acute stroke with dysphagia.
In Vietnam, while research on dysphagia following stroke is mainly focused on methods of screening and diagnosis, to the best of our knowledge, there are no studies available on the effectiveness of these interventions. Therefore, the present study was conducted in an aim to evaluate the effect of food thickeners combined with swallowing exercises in patients with dysphagia following cerebral infarction.
Patients and methods
Research design
The present study adopted a quasi-experimental one-group pre-test/post-test design and a convenience sampling method. For the experimental intervention, patients who suffered a stroke and met the study criteria were treated using swallowing rehabilitation and oral feeding with thickeners. A pre- and post-test were conducted before and 5, 10, and at 15 days following treatment.
Participants and study setting
In the present study, 33 patients who suffered a stroke and were admitted to Hanoi Rehabilitation Hospital (Hanoi, Vietnam) between July, 2020 and May, 2021 were recruited. The mean duration of hospitalization was 2.5 months, the minimum was 3 weeks, and the maximum was 4 months.
The inclusion criteria were as follows: i) An age ≥18 years; ii) first-time ischemic stroke; iii) a Montreal Cognitive Assessment (MoCA) score ≥21 points; iv) a Mann Assessment of Swallowing Ability (MASA) score ≤177; and v) patients must have provided written consent to participate in the study.
The exclusion criteria were the following: i) Patients with cerebral infarction who had respiratory failure and needed to be intubated, with a loss of consciousness, ii) patients with other swallowing disorders, or those with brain damage due to various causes, or those with brain tumors, brain metastases, traumatic brain injury, nervous system infections, encephalitis, or meningitis; iii) patients has epilepsy; and iv) patients with esophageal stenosis and pyloric stenosis.
Intervention and data collection procedure
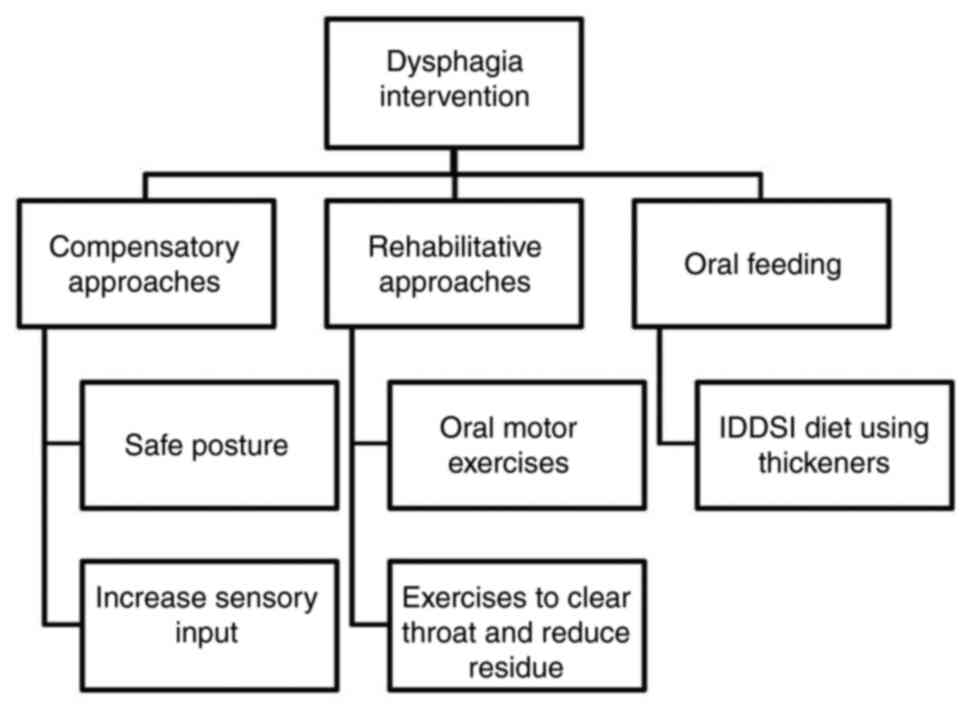
Through clinical evaluation, the speech therapist gathered information about the patient's cognition, motor and sensory impairments, and appropriateness for oral intake, and then developed an individualized rehabilitation program. Dysphagia rehabilitation comprises of compensatory and rehabilitative approaches. Compensatory strategies, including postural adjustments and increasing sensory input are used to reduce symptoms of dysphagia without changing the physiology. Rehabilitative approaches improve swallowing physiology and improve swallow safety and the tolerance of the least restrictive diet, such as oral motor exercises, effortful swallow, Mendelsohn maneuver, supraglottic swallow, Super supraglottic swallow, Masako maneuver and Shaker exercises. The patients received one 35-min session once a day, 5 days a week for 3 weeks. They were also allowed to eat by mouth following The International Dysphagia Diet Standardization Initiative (IDDSI) if considered appropriate. Prerequisites to be tested with oral feeding included: Consciousness, normal vital signs, stable respiratory status (SpO2 of 95%, respiration rates of 12 to 20 breaths per minute, inhalation/exhalation time=1:2, normal lung sounds), and good saliva management. Patients who had pneumonia, wet voice, poor saliva control or no consistencies appeared to be safe for them, were continued as ‘nil by mouth’. The intervention approaches used in the present study are illustrated in Fig. 1.
Intervention materials
The present study used Softia, a Japanese ready-to-use food and beverage thickener supplied by the Asia Food and Nutrition Corporation. Depending on specific drinks and foods, the present study used Softia S, Softia U or Softia G. The MASA data were collected at baseline and at 5, 10, and 15 days following treatment.
Ethical considerations
The families and patients were provided with a detailed explanation about the purpose, rights and obligations while participating in the study. Patients were provided with information about methods and possible discomforts during the study period. The study participants could withdraw from the study at any time.
Instruments
The MASA scale was used to assess the swallowing function of the patients at baseline and after the intervention. It was developed by Mann (11) in 2002 as a screening tool for identifying dysphagia in patients who suffered a stroke.
It is a simple bedside evaluation that carries no risk of aspiration as no feeds of any quantity are introduced to the patient. It is inexpensive and does not require specialist services. Another advantage of this clinical test is that it does not require any special device or radiation exposure.
The MASA scale consists of 24 items, divided into four components as follows: General patient examination, oral preparation phase, oral phase and pharyngeal phase. Each item has a maximum score of 10, and the total score is 200. The cut-off point for dysphagia is 177, and that of aspiration is 169; the severity level of dysphagia and the risk of aspiration was thus determined, as presented in Table I (12,13).
Statistical analysis
The data were analyzed using Stata 14.0 software (StataCorp LLC). Frequencies, percentages and mean/median were calculated to demonstrate the distribution of demographic variables, the severity of swallowing disorder, symptoms of swallowing disorder, the risk of aspiration, the time of intervention and treatment results. Data were analyzed using the Chi-squared statistical test (if <20% of cells had an expected frequency <5) or Fisher's exact test (if >20% of cells had an expected frequency <5) when testing the difference between the two groups. A value of P<0.05 was considered to indicate a statistically significant difference.
Results
Status of dysphagia in the study participants
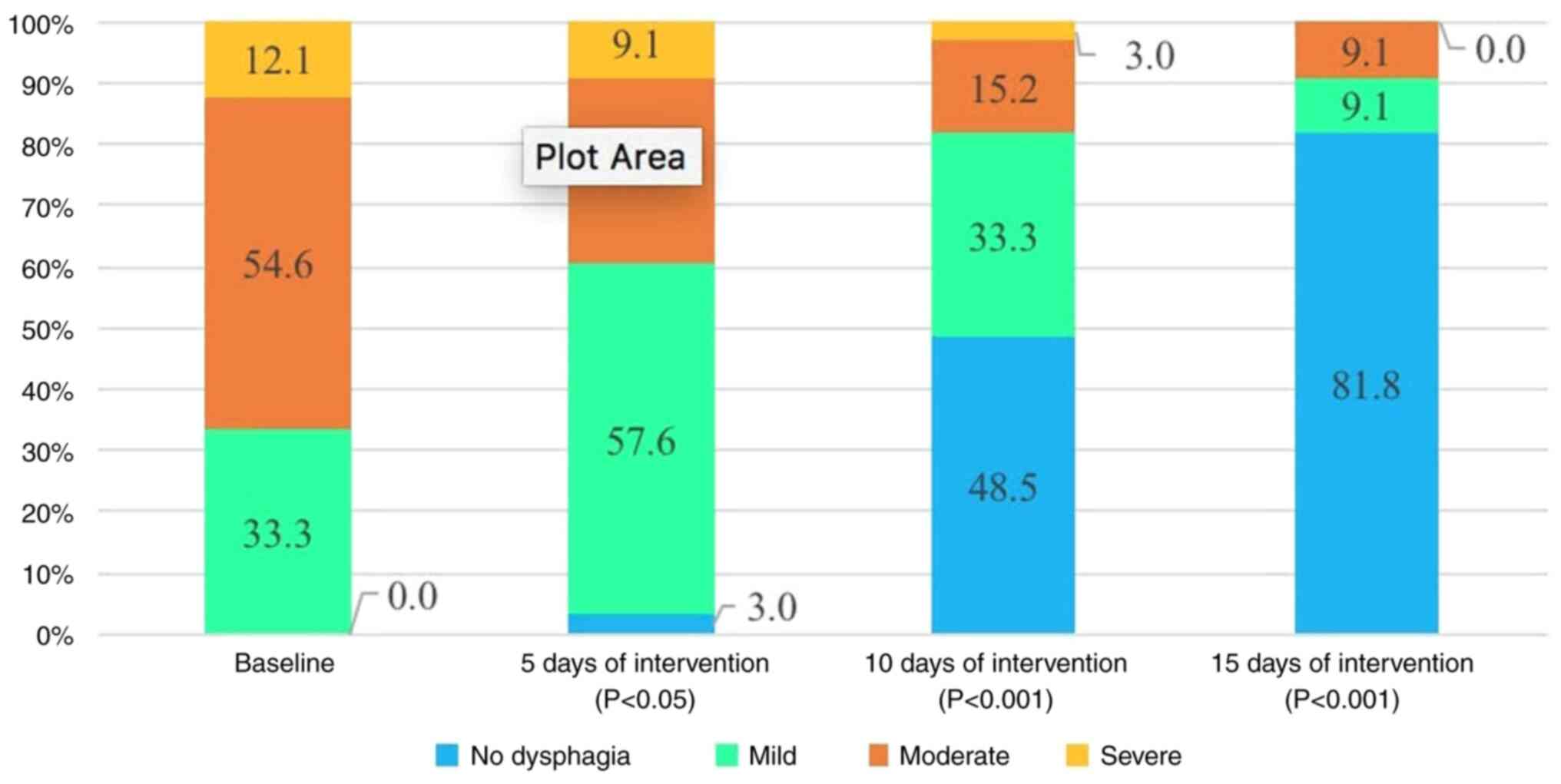
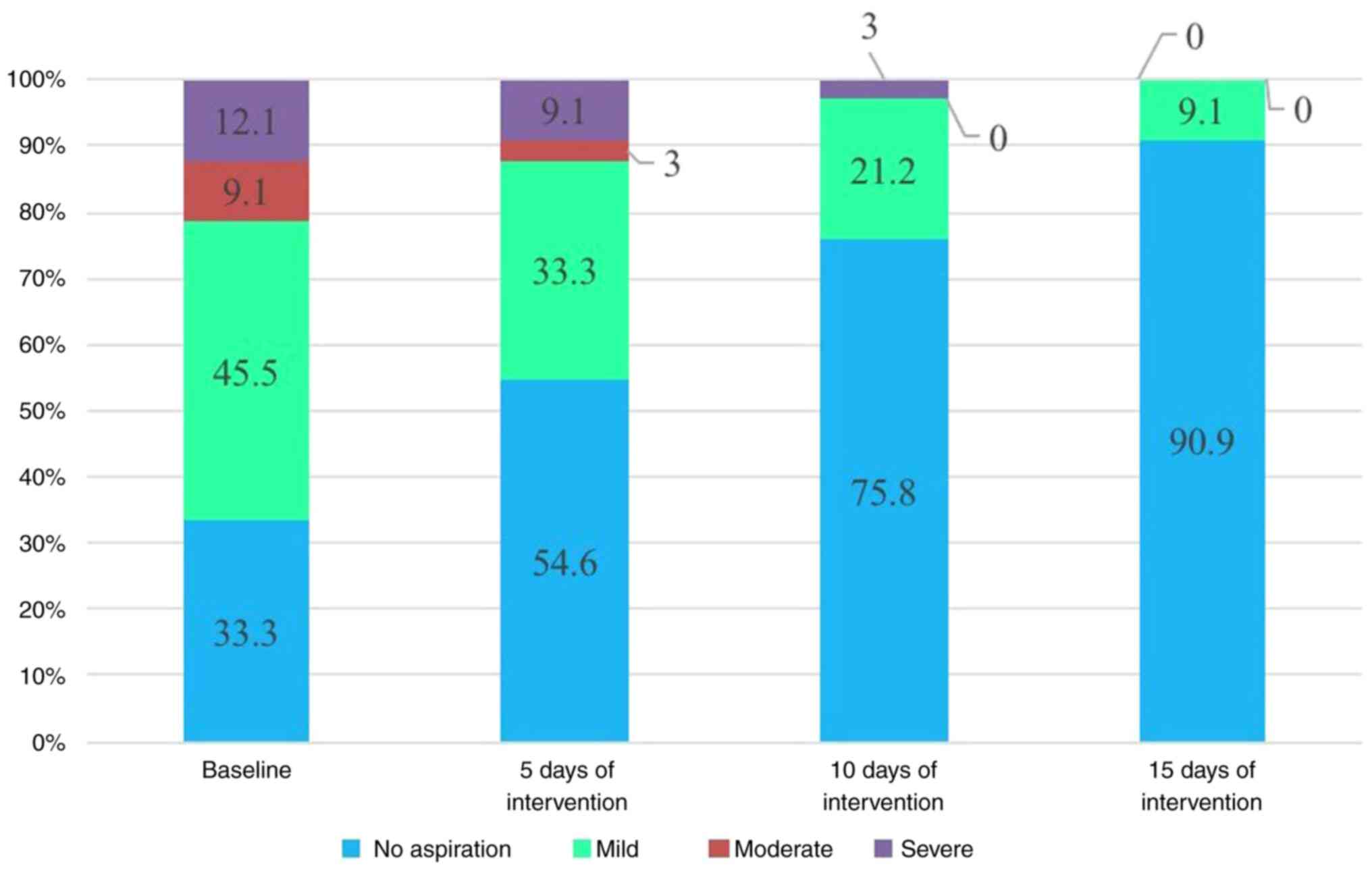
The demographic data of patients who suffered a stroke are presented in Table II. A total of 33 patients who suffered a stroke were selected for the study; there were 22 males and 11 females and 81.8% of the participants were >60 years of age. The majority of the patients had mild to moderate dysphagia (87.9%), and only 4 patients had severe dysphagia (12.1%) (Fig. 2). The most common symptom was cough/choking while swallowing (29 patients, 87.9%). Other symptoms included drooling, food spillage, residue inside the mouth, the sensation of food stuck in the throat or the chest, reduced gag reflex, voice change and ineffective cough. Patients at risk of mild aspiration accounted for a high percentage of 45.5%. A total of 21.2% of patients had a risk of severe and moderate aspiration, and 33.3% of patients did not have a risk of aspiration (Fig. 3). Intervention was implemented as soon as possible. The majority of patients received rehabilitation at an early stage, in <1 month (26 patients,78.8%).
Before and after intervention
The proportion of patients at risk of developing severe aspiration pneumonia decreased from 12.1 to 9.1% after 5 days of treatment. After 15 days of treatment, there were no patients at risk of severe aspiration. The number of patients who were no longer at risk of developing aspiration pneumonia increased from 33.3 to 54.6% after 5 days, to 75.8% after 10 days and to 90.9% after 15 days of treatment (Fig. 3).
The proportion of patients who suffered from severe dysphagia decreased from 12.1 to 9.1% after 5 days, to 3% after 10 days and to 0% after 15 days of treatment. The proportion of patients without swallowing disorder and mild swallowing disorder increased from 33.3 to 60.6% after 5 days of treatment, to 81.8% after 10 days and to 90.9% after 15 days of treatment (P<0.05). The percentage of patients whose dysphagia resolved after 10 days was 48.5% and after 15 days this number was 81.8% (Fig. 2).
The rate of swallowing disorders after 15 days of intervention was 18.2%. In particular, a comparison between groups regarding the time of intervention revealed that the rate of swallowing disorders in the early intervention group <1 week (0%) and 1-4 weeks (0%) was lower than that in the intervention group at 1-2 months (80%) and >2 months (100%), with the difference being statistically significant (P<0.001) (Table III).
Table IIIAssociation between the onset of intervention and outcomes in the patients following 15 days of intervention. |
Following treatment, all symptoms of dysphagia improved. The rate of choking when swallowing decreased from 87.9 to 9.1%. Drooling and food spillage symptoms decreased from 63.6 and 66.7 to 12.1%.
Discussion
In 2000, Mann et al (14) conducted a study on 128 patients who suffered a stroke who were clinically evaluated by the MASA scale and the results were compared with VFS. Patients were followed-up for 6 months following the stroke; the MASA scale was proven to be valuable compared with VFS in diagnosing dysphagia with a sensitivity of 73% and specificity of 89%; the diagnosis of aspiration with a specificity of 93% and specificity of 67% (14).
In the present study, the severity of dysphagia was evaluated according to the MASA scale. The results revealed that 33.3% of the patients had mild dysphagia, 54.6% had moderate dysphagia and 12.1% had severe dysphagia. The clinical symptoms of swallowing disorders included coughing and choking during and after eating (87.9%), food spillage (66.7%), drooling (63.3%), food residue inside the mouth (60.6%), the sensation of food being stuck in the throat or chest (57.6%), decreased gagging reflex (54.6%) and voice change after swallowing (33.3%). The study by Terré and Mearin (15) revealed that 47% of patients with dysphagia coughed while eating, 44% had decreased gag reflex, and 13% experienced a change in voice.
According to previous research, cough and voice change after swallowing are key clinical signs of dysphagia suggesting aspiration. According to the study by Daniels et al (16), voice change and wet voice after swallowing had a sensitivity and specificity of 38.1 and 85.3%, and cough after swallowing had a sensitivity of 38.5% and specificity of 84.8%. When combining these two symptoms, sensitivity and specificity increased to 92.3 and 66.7%. Although they are not the gold standard for diagnosing swallowing disorders, they are easy to use and can help predict the risk of aspiration pneumonia. If patients are evaluated and treated at an early stage, the risk of aspiration and other complications from dysphagia will then be reduced. Some cases of voice change after swallowing are difficult to recognize and the examiner needs to re-examine several times (16,17-18).
The results of the present study also demonstrated that 45.5% of patients had a low risk of aspiration, 12.1% with high risk and 9.1% with medium risk. According to the study by Mann et al (14) on 128 patients who were clinically evaluated within 3 days following a stroke, 51% of the patients suffered from aspiration. The patients were assessed by VFS within 10 days after the stroke and the rate of aspiration was 22% . Another study demonstrated that approximately one-third of patients who suffered a stroke aspirated on VFS. Among the patients that aspirated, one-third developed pneumonia and half of them aspirated silently (19).
Swallowing rehabilitation includes swallowing exercises and maneuvers, postural and compensation techniques, diet and environmental modification, and alternative feeding (20). It has been proven to be a simple and valid approach to reducing the risk of aspiration. Lazarus et al (21) demonstrated that supraglottic swallow was effective in closing the vocal cords to protect the airway during swallowing, especially when combined with the Mendelsohn maneuver. The study by Bülow et al (22) demonstrated that effortful swallow reduced the depth of airway infiltration, and should be combined with exercises to increase the strength and range of motion of the tongue. Shaker et al (23) performed a study on 24 patients with dysphagia and the results revealed that the Shaker exercise increased the opening of the upper esophageal sphincter and anterior movement of the larynx, reduced residue in pyriform sinus and aspiration after swallowing.
Softia is a ready-to-use food and beverage thickener that was developed in Japan. Softia rapidly increases the viscosity of the liquid and maintains a stable consistency. The advantage of Softia is that it dissolves rapidly and is not affected by the enzyme amylase in saliva. With Softia thickener, the IDDSI diet and compensatory techniques, such as safe posture, the patient can actively control the flow of the bolus, thereby improving their swallowing function.
The present study demonstrated that the proportion of patients with severe dysphagia decreased to 0% following 15 days of treatment. The proportion of patients who no longer had swallowing disorder and mild swallowing disorder increased to 90.9% after 15 days of treatment.
In the present study, after applying swallowing rehabilitation exercises in combination with the IDDSI diet using thickeners, there was an improvement in the risk of aspiration specifically as follows: The proportion of patients at risk of severe aspiration decreased after 5 days of treatment from 12.1 to 9.1%. Following 15 days of treatment, there were no patients at risk of severe aspiration. The number of patients who were no longer at risk of aspiration increased after 5 days of treatment from 33.3 to 54.6%, to 75.8% after 10 days and to 90.9% after 15 days of treatment.
According to the study by Clavé et al (7) penetration into the laryngeal vestibule occurred most often when swallowing food at liquid viscosity (21.6 mPa.s); this decreased when the subject was given nectar (295.0 mPa.s), and further with pudding consistency (3682.2 mPa.s). Rofes et al (9) also reported a statistically significant result in which increasing the consistency of food bolus from liquid to pudding reduced the rate of aspiration and aspiration pneumonia in 98.9% of patients.
Kuhlemeier et al (6) studied >190 subjects with dysphagia associated with different causes ranging from mild to moderate by VFS. The results revealed that the rate of aspiration was higher when drinking thin liquid from a cup than when having extra-solid food with a spoon. Similar results proved that swallowing safety was improved when using xanthan gum as a thickener, as there was a significant reduction in aspiration from 35.3% with thin liquids to 13.7% with nectar and 9.3% with spoon-thick form). Another study was conducted on 61 patients post-stroke; when increasing the food bolus consistency from a thin liquid to spoon-thick form (very thick), the results revealed a significant reduction in the rate of aspiration into the larynx, and no patient had any symptoms of aspiration following intervention (8).
In the present study, following treatment, all symptoms of dysphagia improved. All the changes in symptoms were statistically significant (P<0.05). Thus, the combination of swallowing rehabilitation exercises with the use of thickeners to adjust the diet for patients with dysphagia contributed to improving symptoms and helping patients to be more confident. They no longer felt concerned after choking and coughing several times, thereby being motivated to practice.
The results of the present study demonstrated that the number of patients whose dysphagia resolved after 10 days was 48.5% and after 15 days this number was 81.8%. The approach of swallowing intervention by combining swallowing exercises with adjusting the food consistency with thickeners proved to be very effective. According to the study by Kwakkel et al (24), patients would recover the most during the first 6 months after a stroke). Therefore, the sooner the intervention, the better the prognosis of patients recovering from dysphagia. Thus, the onset of intervention is one of the prognostic factors for patients. Patients who suffer a stroke need to be screened for swallowing disorders and received treatment as soon as they are in the intensive care unit.
The present study had certain limitations which should be mentioned. Firstly, the use of a single-group design, and lack of a control group suggest that the results should be generalized with caution. Secondly, the present study only used the MASA scale, a clinical evaluation to assess dysphagia. Another limitation of the present study was the small sample size. The present study was conducted with a limited number of participants, which may affect the generalizability and reliability of the findings. According to the results of the present study, the authors propose the following recommendations: i) Future studies are required to employ randomized controlled trials to enhance the validity of the conclusion; and ii) further studies are require to enhance the validity of the study results, and future studies may use medical devices to objectively measure the results of the intervention, such as VFS.
In conclusion, as demonstrated in the present study, the majority of the patients who suffered a stroke had mild and moderate dysphagia. A combination of swallowing rehabilitation exercises and using thickeners to adjust the diet for patients with dysphagia helped reduce the severity of swallowing dysfunction, and the rate of aspiration and improved all symptoms, particularly choking. Patients who received early intervention had a better prognosis and recovery from dysphagia.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors' contributions
VMP, TVN and THL were involved in the conception and design of the study, were performed the statistical analysis of the data. VMP, TVN and TTHN were involved in the investigative aspects of the study. VMP, TVN and THL were involved in the interpretation of the data. VMP, TVN, TTHN and THL were involved in the writing of the origional draft of the manuscript, and in the writing, reviewing and editting of the manuscript. All authors read and agreed to the published version of the manuscript. VMP and THL confirm the the authenticity of all the raw data.
Ethics approval and consent to participate
The present study was approved by the Hanoi Medical University Institutional Ethical Review Board under Decision No. 268/GCN-HDDDNCYSH-DHYHN, dated June 8, 2020. All patients were provided a written consent to participate in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
|
Krishnamurthi RV, Ikeda T and Feigin VL: Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: A systematic analysis of the global burden of disease study 2017. Neuroepidemiology. 54:171–179. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Carr C, Kahn L, Mathkour M, Biro E, Bui CJ and Dumont AS: The shifting burden of neurosurgical disease: Vietnam and the middle-income nations. Neurosurg Focus. 45(E12)2018.PubMed/NCBI View Article : Google Scholar | |
|
Takizawa C, Gemmell E, Kenworthy J and Speyer R: A systematic review of the prevalence of oropharyngeal dysphagia in stroke, Parkinson's disease, Alzheimer's disease, head injury, and pneumonia. Dysphagia. 31:434–441. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Vesey S: Dysphagia and quality of life. Br J Community Nurs. 18:S14–19. 2013.PubMed/NCBI View Article : Google Scholar | |
|
Newman R, Vilardell N, Clavé P and Speyer R: Effect of bolus viscosity on the safety and efficacy of swallowing and the kinematics of the swallow response in patients with oropharyngeal dysphagia: White paper by the European society for swallowing disorders (ESSD). Dysphagia. 31:232–249. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Kuhlemeier KV, Palmer JB and Rosenberg D: Effect of liquid bolus consistency and delivery method on aspiration and pharyngeal retention in dysphagia patients. Dysphagia. 16:119–122. 2001.PubMed/NCBI View Article : Google Scholar | |
|
Clavé P, Arreola V, Romea M, Medina L, Palomera E and Serra-Prat M: Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin Nutr. 27:806–815. 2008.PubMed/NCBI View Article : Google Scholar | |
|
Diniz PB, Vanin G, Xavier R and Parente MA: Reduced incidence of aspiration with spoon-thick consistency in stroke patients. Nutr Clin Pract. 24:414–418. 2009.PubMed/NCBI View Article : Google Scholar | |
|
Rofes L, Arreola V and Clavé P: The volume-viscosity swallow test for clinical screening of dysphagia and aspiration. Nestle Nutr Inst Workshop Ser. 72:33–42. 2012.PubMed/NCBI View Article : Google Scholar | |
|
Jongprasitkul H and Kitisomprayoonkul W: Effectiveness of conventional swallowing therapy in acute stroke patients with Dysphagia. Rehabil Res Pract. 2020(2907293)2020.PubMed/NCBI View Article : Google Scholar | |
|
Mann G: MASA, the mann assessment of swallowing ability. Vol. 1 New York, NY: Cengage Learning; (2002). | |
|
Antonios N, Carnaby-Mann G, Crary M, Miller L, Hubbard H, Hood K, Sambandam R, Xavier A and Silliman S: Analysis of a physician tool for evaluating dysphagia on an inpatient stroke unit: The modified mann assessment of swallowing ability. J Stroke Cerebrovasc Dis. 19:49–57. 2010.PubMed/NCBI View Article : Google Scholar | |
|
Kwon S, Sim J, Park J, Jung Y, Cho KH, Min K, Kim MY, Kim KM and Im SH: Assessment of aspiration risk using the mann assessment of swallowing ability in brain-injured patients with cognitive impairment. Front Neurol. 10(1264)2019.PubMed/NCBI View Article : Google Scholar | |
|
Mann G, Hankey GJ and Cameron D: Swallowing disorders following acute stroke: Prevalence and diagnostic accuracy. Cerebrovasc Dis. 10:380–386. 2000.PubMed/NCBI View Article : Google Scholar | |
|
Terré R and Mearin F: Oropharyngeal dysphagia after the acute phase of stroke: Predictors of aspiration. Neurogastroenterol Motil. 18:200–205. 2006.PubMed/NCBI View Article : Google Scholar | |
|
Daniels SK, Brailey K, Priestly DH, Herrington LR, Weisberg LA and Foundas AL: Aspiration in patients with acute stroke. Arch Phys Med Rehabil. 79:14–19. 1998.PubMed/NCBI View Article : Google Scholar | |
|
Warms T and Richards J: ‘Wet Voice’ as a predictor of penetration and aspiration in oropharyngeal dysphagia. Dysphagia. 15:84–88. 2000.PubMed/NCBI View Article : Google Scholar | |
|
Murray J, Langmore SE, Ginsberg S and Dostie A: The significance of accumulated oropharyngeal secretions and swallowing frequency in predicting aspiration. Dysphagia. 11:99–103. 1996.PubMed/NCBI View Article : Google Scholar | |
|
McCullough GH, Rosenbek JC, Wertz RT, McCoy S, Mann G and McCullough K: Utility of clinical swallowing examination measures for detecting aspiration post-stroke. J Speech Lang Hear Res. 48:1280–1293. 2005.PubMed/NCBI View Article : Google Scholar | |
|
Palmer JB, Pelletier CA and Matsuo K: Rehabilitation of patients with swallowing disorders. In: Braddom R. L., Chan L., Harrast M. A. et al., Editors. Physical Medicine and Rehabilitation. 4th. Philadelphia: Elsevier Saunders, 2011. | |
|
Lazarus CL, Logemann JA, Rademaker AW, Kahrilas PJ, Pajak T, Lazar R and Halper A: Effects of bolus volume, viscosity, and repeated swallows in nonstroke subjects and stroke patients. Arch Phys Med Rehabil. 74:1066–1070. 1993.PubMed/NCBI View Article : Google Scholar | |
|
Bülow M, Olsson R and Ekberg O: Videomanometric analysis of supraglottic swallow, effortful swallow, and chin tuck in patients with pharyngeal dysfunction. Dysphagia. 16:190–195. 2001.PubMed/NCBI View Article : Google Scholar | |
|
Shaker R, Easterling C, Kern M, Nitschke T, Massey B, Daniels S, Grande B, Kazandjian M and Dikeman K: Rehabilitation of swallowing by exercise in tube-fed patients with pharyngeal dysphagia secondary to abnormal UES opening. Gastroenterology. 122:1314–1321. 2002.PubMed/NCBI View Article : Google Scholar | |
|
Kwakkel G, Kollen B and Lindeman E: Understanding the pattern of functional recovery after stroke: Facts and theories. Restor Neurol Neurosci. 22:281–299. 2004.PubMed/NCBI |








