



Circulating tumor DNA serial monitoring of relapse and responses to tislelizumab immunotherapy as second‑line monotherapy for metastatic esophageal squamous cell carcinoma: A prospective study
- Authors:
- Published online on: February 9, 2024 https://doi.org/10.3892/mco.2024.2727
- Article Number: 29
-
Copyright: © He et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
Introduction
Esophageal squamous cell carcinoma (ESCC) is the predominant (90%) histological type of Esophageal cancer. The prognosis of advanced ESCC is poor, with a median overall survival (OS) of ~1 year, highlighting the great need for new therapies (1,2) Recent clinical results support the use of new immune checkpoint blockers, such as anti-programmed cell death 1 (PD-1) and PD-1 ligand 1 (PD-L1) antibodies, as part of the antitumor treatments in several cancer types, including ESCC. These inhibitors are recommended to be used either as second-line monotherapy or in combination with platinum doublet chemotherapy in patients with tumors expressing PD-L1 at any level in ESCC (3-8). Such treatments would be facilitated by the selection of biomarkers that can sensitively and noninvasively detect early responses and predict prognoses. The reality is that conventional clinical assessment and imaging, such as endoscopy, endoscopic ultrasound and computed tomography (CT), are not sufficiently robust methods of gauging treatment response to anti-PD-1/PD-L1 therapy, such as pseudoprogression, which manifests in delayed clinical responses in certain patients, consisting of an initial increase in tumor size, which is subsequently followed by tumor shrinkage due to tumor immune cell infiltration (9,10). These results demonstrate that clinical assessment and imaging cannot always reliably predict clinical benefits and survival in patients who received immunotherapy. Accordingly, there is an unmet clinical need to identify biomarkers that can sensitively detect early progression and predict prognosis in patients with ESCC receiving anti-PD-1 immunotherapy. Circulating tumor DNA (ctDNA) is a new biomarker that has been mostly investigated as a tool for liquid biopsy, as it harbors mutations similar to those in DNA extracted from tumor biopsies (11-13). Of note, ctDNA detection techniques are quantitative, and changes in ctDNA levels during chemotherapy and targeted therapy have been associated with tumor response or progression in several tumor types; ctDNA levels may predict outcomes for patients undergoing esophagectomy for ESCC (14-16). However, to the best of our knowledge, no previous study has applied ultrasensitive next-generation sequencing (NGS) methods to detect ctDNA changes in patients with ESCC receiving anti-PD-1 monotherapy as a second-line therapy. The present study reported on the deep sequencing of 425 cancer-related genes in 43 ctDNA samples collected before treatment and at different time-points during treatment with tislelizumab (an anti-PD-1 drug) in 12 patients with ESCC. It was demonstrated that ctDNA sequencing is promising for predicting the response and prognosis after treatment with tislelizumab as a second-line monotherapy for advanced ESCC.
Patients and methods
Subjects and study procedure
Our research center is one of the sub-centers of the RATIONALE-302(17) study (ClinicalTrials.gov identifier no. NCT03430843), of which 20 subjects were screened and 15 were enrolled, of which 12 patients were eligible for this exploratory study at Zhejiang Cancer Hospital (Hangzhou, China) between March 2018 and September 2020, whose tumor tissue or plasma was available for NGS. Eligible patients were aged 18-73 years and previously treated with systematic chemotherapy for stage IV ESCC, who were being treated with tislelizumab immuno-monotherapy 200 mg intravenous drip every 3 weeks until disease progression. Specific inclusion and exclusion criteria were those of the RATIONALE-302 study (17). This study was approved by the Institutional Review Board of Zhejiang Cancer Hospital (Hangzhou, China) and all patients provided written informed consent. The study was conducted in accordance with the established ethical standards of the institutional and/or national research committee, as outlined in the Declaration of Helsinki.
Radiographic data and clinical outcomes
Patients underwent CT imaging at a follow-up visit at every 6-8 weeks during immunotherapy and chest and abdominal CT scans were evaluated according to Response Evaluation Criteria in Solid Tumours (RECIST 1.1) (18), by a radiologist blinded to circulating cell-free DNA (cfDNA) data. Progression-free survival (PFS) was defined as the interval between treatment initiation and the date of disease progression or death from any cause, whichever occurred earlier. Overall survival (OS) was defined as the time interval from treatment initiation to death from any cause. A censor date of June 30, 2021 was applied if no endpoint was met.
Tumor and blood sample collection
Fresh ESCC tumor samples from patients undergoing esophagogastroscopy were obtained from 12 patients before immunotherapy. A total of 35 blood samples for ctDNA were obtained at baseline, when patients achieved a status of partial response (PR) or stable disease (SD), or after progressive disease (PD) from March 2018 through to September 2020. Tumor samples were subjected to pathological diagnosis, graded according to the World Health Organization system (19) and then prepared into formalin-fixed and paraffin-embedded (FFPE) blocks. Peripheral blood (8-10 ml) was collected from each patient at each time-point in EDTA-coated tubes (BD Biosciences), and plasma was separated within 2 h after peripheral blood collection. All samples were sent to the centralized testing center of Nanjing Geneseeq Technology, Inc. (Nanjing, China) for targeted NGS.
DNA extraction and library construction
Genomic DNA from FFPE tissues was extracted using a QIAamp DNA FFPE Tissue Kit (Qiagen GmbH). DNA from white blood cells (WBC) was extracted with the DNeasy Blood & Tissue Kit (Qiagen GmbH) and sequenced as normal controls to distinguish germline variations. Plasma-derived cfDNA was extracted using the QIAamp Circulating Nucleic Acid Kit (Qiagen GmbH). DNA was quantified with a Qubit 3.0 (Thermo Fisher Scientific, Inc.) and the quality was assessed using a Nanodrop 2000 (Thermo Fisher Scientific, Inc.). FFPE and WBC-derived DNA was sheared into 300-350 bp fragments using a Covaris M220 instrument (Covaris, Inc.). cfDNA or fragmented genomic DNA was prepared using a KAPA Hyper Prep Kit (KAPA Biosystems) as previously described (20). In brief, the DNA was subjected to end repair, A-tailing and adaptor ligation. DNA was then amplified and purified. A customized NGS panel containing 425 cancer-related genes was used for library enrichment. The captured libraries were amplified, purified and quantified. All the experimental procedures were performed at Nanjing Geneseeq Technology, Inc.
Library sequencing and bioinformatics analysis
The prepared library was sequenced using a HiSeq4000 platform (Illumina, Inc.). The mean coverage depth was 150x µm for WBC controls and 800x µm for tissue samples. For cfDNA samples, the mean coverage sequencing depth was 5,000x. Base calling was performed on a bcl2fastq v2.16.0.10 (Illumina, Inc.) to generate sequence reads in the FASTQ format (Illumina 1.8+ encoding). Quality control was performed using the Trimmomatic software version 0.40 (https://github.com/usadellab/Trimmomatic). High-quality reads were aligned to the human genome (hg19; Genome Reference Consortium Human ref. 37) using Burrows-Wheeler Aligner 0.7.12 (https://github.com/lh3/bwa/tree/master/bwakit). The data were further processed using Picard 1.119 (https://github.com/broadinstitute/picard/releases/latest) and the Genome Analysis Toolkit (GATK; version 3.4.0; https://software.broadinstitute.org/gatk).
Single nucleotide variants (SNVs) and short insertions/deletions (indels) were identified using VarScan2 and HaplotypeCaller/UnifiedGenotyper in GATK, with a minimum mutant allele frequency cut-off of 0.5% for tissue, 0.3% for cfDNA and a minimum of three unique mutant reads with good quality scores. All SNVs/indels were annotated using ANNOVAR (default version; https://bioweb.pasteur.fr/packages/pack@annovar@24.10.2019) and manually checked using the Integrative Genomics Viewer version 2.10.3 (https://igv.org). Gene fusions/rearrangements were identified using FACTERA version 1.4.4 (https://factera.stanford.edu/download.php) and copy number gain or loss was analyzed using ADTEx version 2.0 (https://sourceforge.net/projects/adtex). The log2 ratio cutoff defined for copy number gain was 2.0 for tissue and 1.6 for cfDNA. A log2 ratio cutoff defined for copy number loss was 0.6 for all sample types. Tissue tumor mutation burden (tTMB) was calculated according to Fang's study (21). High-level tTMB (tTMB-H) was defined as ≥10 mutations/Mb (mut/Mb) and <10 mut/Mb was defined as tTMB-L.
ctDNA monitoring and MMPM analysis
A longitudinal ctDNA analysis was performed and the mutant molecules per milliliter of plasma (MMPM) were measured, which quantifies ctDNA for all variants. The overall MMPM for each sample was defined as the mean MMPM (mMMPM) across SNVs and indels, which was calculated as previously described (22,23). In brief, the mMMPM was calculated from the mean allele fraction (mAF) of variants by multiplying by the extracted mass (ng), dividing by the plasma volume (ml) and adjusting by a factor of 330 haploid human genome equivalents per ng:
 |
∆mMMPM was defined as the percentage change of mMMPM in plasma at the first monitoring time-point after the first infusion of tislelizumab (ranging from cycles 2 to 6) since baseline for each patient:
 |
Statistical analysis
Quantitative data are presented as the median (range) or n (%). Proportion comparisons between the groups were performed using Fisher's exact test. Kaplan-Meier curves were used to perform the survival analysis. Genes with mutations that were significantly associated with PFS and OS were screened using univariate Cox models. A two-sided P<0.05 was considered statistically significant for all tests unless indicated otherwise. All analyses were performed using R software version 3.6.3 (https://cran.r-project.org/bin/windows/base/old/3.6.3/).
Results
Patient characteristics
Between March 2018 and September 2020, 15 patients who received tislelizumab as a second-line treatment for advanced ESCC in the RATIONALE-302 study (17) were recruited for the present study. Among them, 12 patients had endoscopic biopsy samples taken before tislelizumab immunotherapy, as well as plasma samples before and after every 2-3 (6-9 weeks) treatment cycle and disease progression. These 12 patients were included in the subsequent analysis. All 12 patients had interpretable data at the pretreatment time-point and 10 patients (83.3%) had interpretable data of NGS at the dynamic time-points and were used for analyses. The median age of the patients was 62.5 years (range, 46-73 years). There were 11 men (91.7%), nine current or former heavy drinkers (75.0%) with >1 l of liquor per day. The Eastern Cooperative Oncology Group performance status (24) of all the 12 patients was 0-1. Among these 12 patients, a total of four patients (33.3%) had undergone surgery and nine patients (75.0%) had received local radiotherapy, one of them had undergone both surgery and radiotherapy. Of the 12 patients, nine (75%) had evaluable lymph node metastases, six (50%) had lung metastases and two (16.7%) had liver metastases. All patients received tislelizumab as the second-line treatment. A total of six patients (50.0%) received ≥12 cycles of tislelizumab. The overall response rate was 33.3%. After a median follow-up of 19.3 months, eight patients (66.7%) exhibited confirmed tumor progression, of whom six (50.0%) died (Table I). The median PFS of the 12 patients treated with tislelizumab was 7.9 months (Fig. 1A) and the median OS was 17.6 months (Fig. 1B). Tumor evaluation was performed after every 2 injections of tislelizumab at 6 weeks of treatment for all patients, except for one patient with severe immune-related thrombocytopenia, who died quickly after only one injection of tislelizumab. This patient only underwent endoscopic biopsy and plasma samples were taken before treatment and were included in the following ctDNA analyses. Of the 12 patients with ESCC in the present study, almost all clinical characteristics (such as age, sex, treatments, cycles of treatment and number of metastatic organs) were not significantly associated with clinical response and outcome (data not shown), except for liver metastasis. The present results showed that patients with liver metastasis had a significantly shorter mPFS (1.4 vs. 11.7 months; P=0.037) (Fig. 1C) and a tendency of shorter OS (13.2 vs. 17.6 months; P=0.560) (Fig. 1D). Table I describes the population characteristics and clinical response to tislelizumab immunotherapy of the patients of this study.
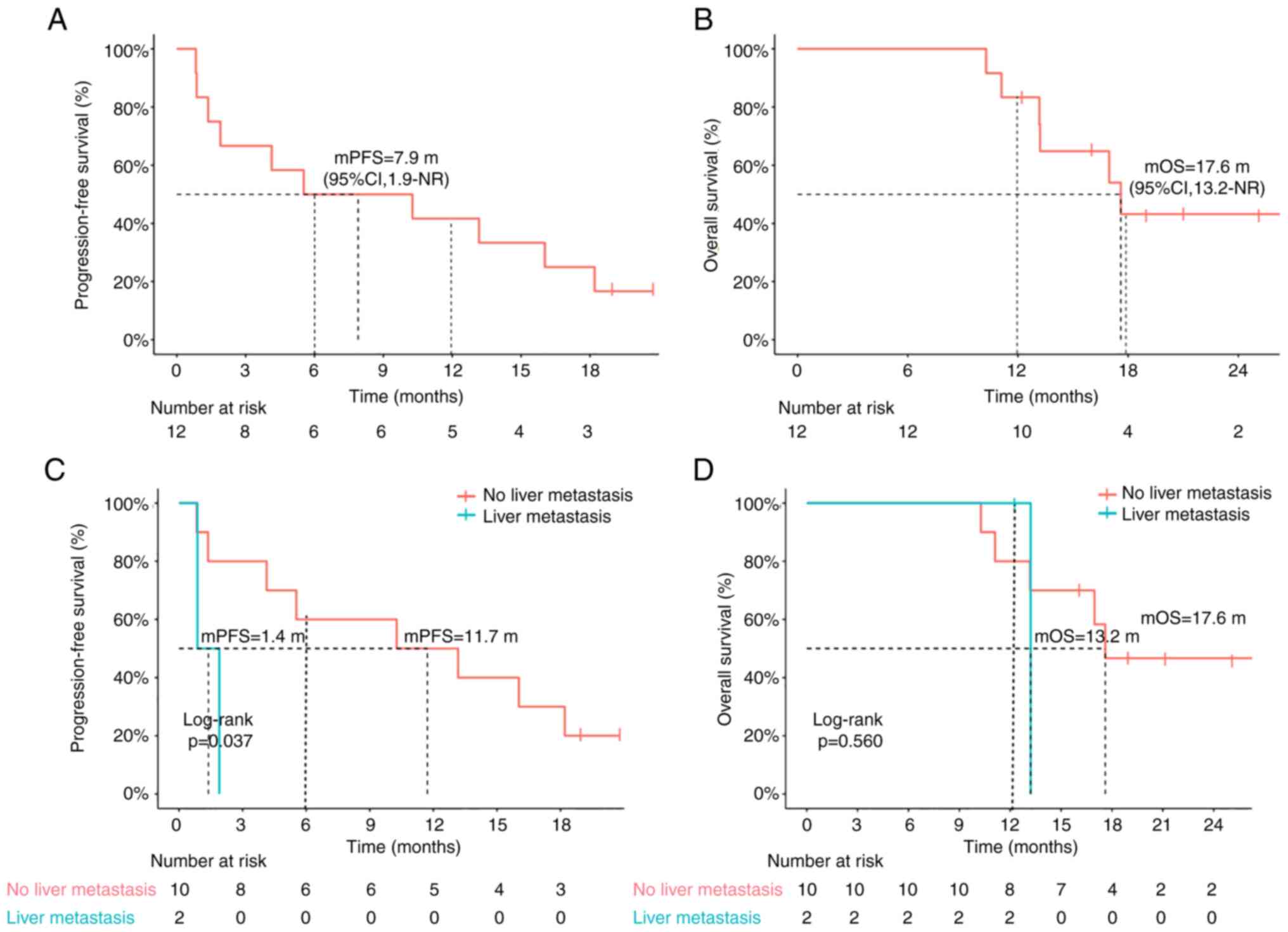
Table IClinical characteristics of patients receiving tislelizumab therapy and their tumor response in the present study (n=12). |
Genomic profiling of ESCC from pre-treatment tumor DNA and ctDNA detection
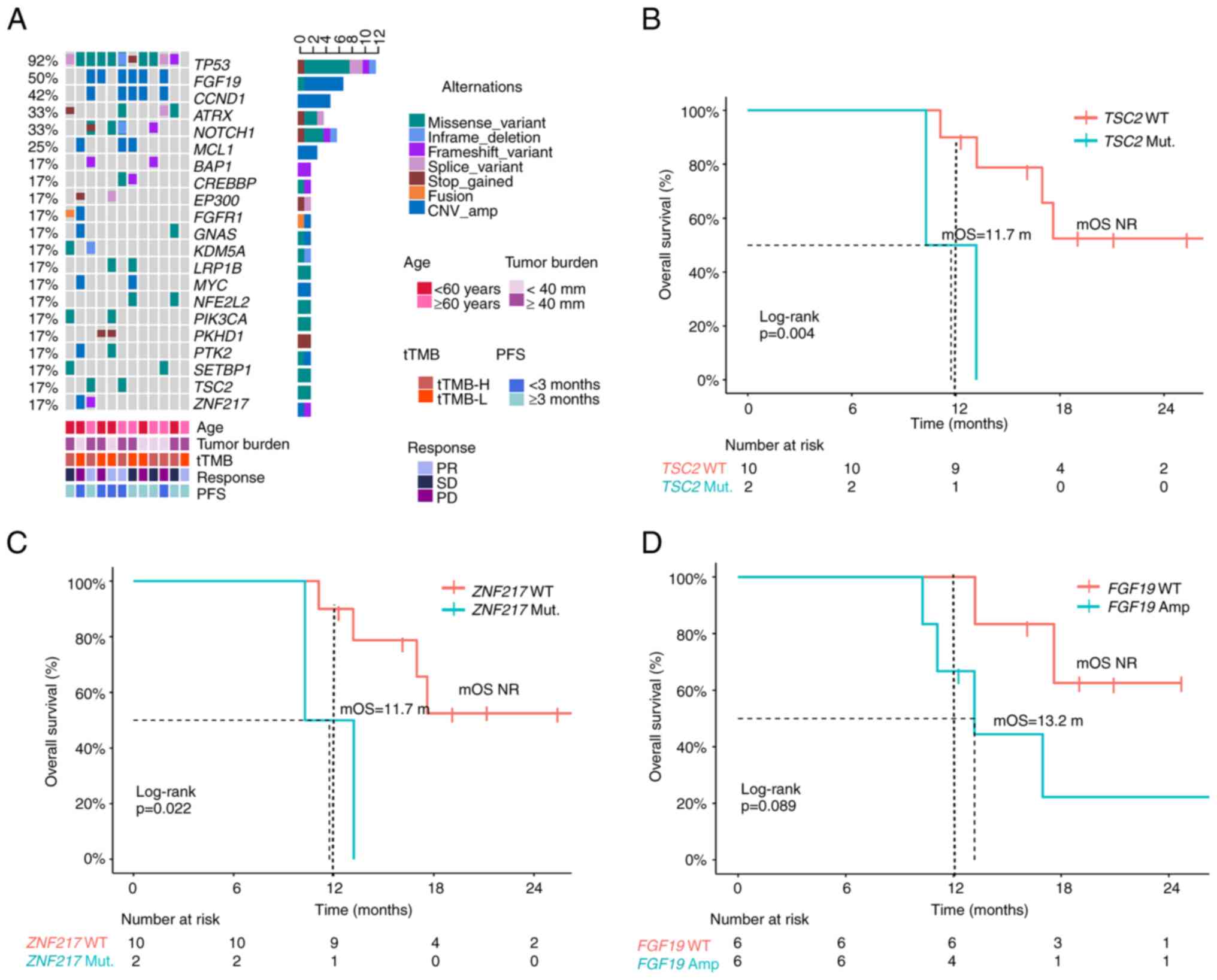
Tumor tissues were available from all 12 patients and were subjected to targeted sequencing of 425 cancer-associated genes. Tumor mutation profiles included high-frequency alterations in tumor protein (TP)53 and cell cycle genes, such as fibroblast growth factor (FGF)19 and cyclin (CCN)D1 (Fig. 2A). According to the Kaplan-Meier survival analysis, the median OS for TSC complex subunit 2 (TSC2) and zinc finger protein 217 (ZNF217) gene mutation was significantly shorter than that for TSC2 [11.7 months vs. not reached (NR), P=0.004, Fig. 2B] or ZNF217 wide type (11.7 months vs. NR, P=0.022, Fig. 2C), while this trend was not significant for PFS. Furthermore, patients with FGF19 gene amplification had a slightly longer PFS (Fig. S1A) and OS (Figs. 2D and S1B) than patients with FGF19 gene wild-type, but the differences were not significant. However, when patients were stratified by the tTMB, patients with tTMB-H had longer PFS and OS than patients with tTMB-L, although no significant differences were obtained (PFS: 10.8 vs. 7.2 months, P=0.750; OS: 17.0 vs. 13.2 months, P=0.680) (Fig. S1C and D).
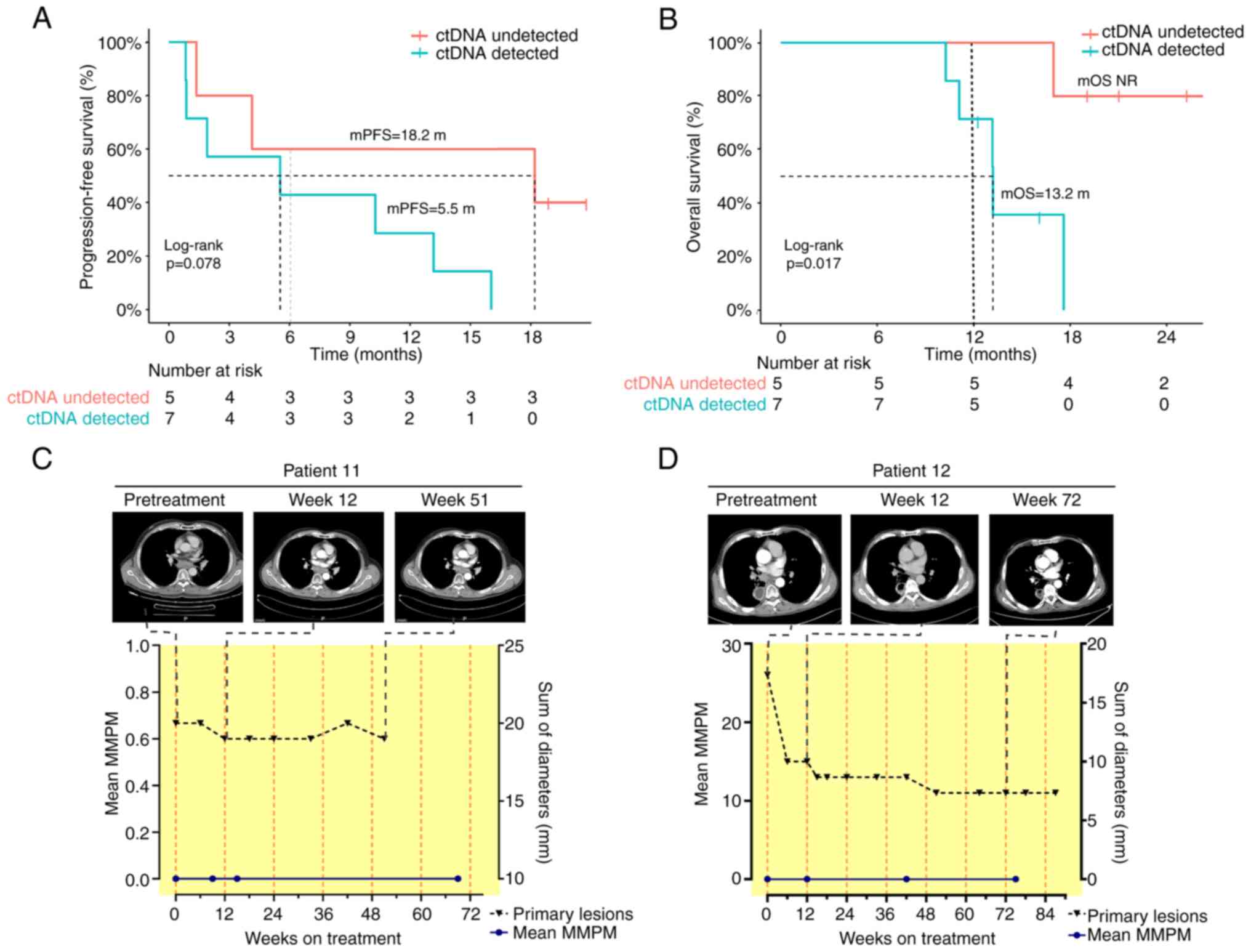
Subsequently, pretreatment ctDNA levels were analyzed in 12 patients for whom baseline plasma samples were available. Table SI shows the ctDNA results for all 35 plasma samples collected by NGS for each patient. ctDNA was detected in 7/12 (58.3%) patients at baseline. Patients with undetectable ctDNA at baseline showed prolonged OS compared to those with detected ctDNA (NR vs.13.2 months; P=0.017) and had a better tendency in PFS (18.2 vs. 5.5 months; P=0.078) (Fig. 3A and B). The mMMPM in these 10 patients at baseline was 91.68 (range: 0-462.72). ctDNA remained undetectable in two patients during the entire serial monitoring.
ctDNA dynamics and treatment efficacy
Three patterns of ctDNA molecular status were observed in the 10 patients who had plasma samples taken after tislelizumab treatment.
The first pattern, seen in two of the ctDNAs undetectable in the whole serial monitoring (Patients 11 and 12), was consistent with radiologic PR or SD for >1 year up to the end of follow-up time (Fig. 3C and D). In these two cases, tumor-specific variants were undetectable during serial monitoring of tislelizumab immunotherapy. The follow-up duration for these two patients were 12 and 17 months, respectively, and no disease progression had occurred at the last follow-up.
In the second pattern, ctDNA levels displayed a relatively obvious rise (defined as ∆mMMPN ≥20%) 2-6 cycles after therapeutic initiation. However, two patients with ∆mMMPN ≥20% showed no clinical benefit. One patient exhibited PD and another patient showed SD with a PFS of <4 months. As a representative case, ctDNA levels in patient 04 continued to rise from the time of initiation of tislelizumab immunotherapy, which is consistent with radiographically confirmed PD (Fig. 4A).
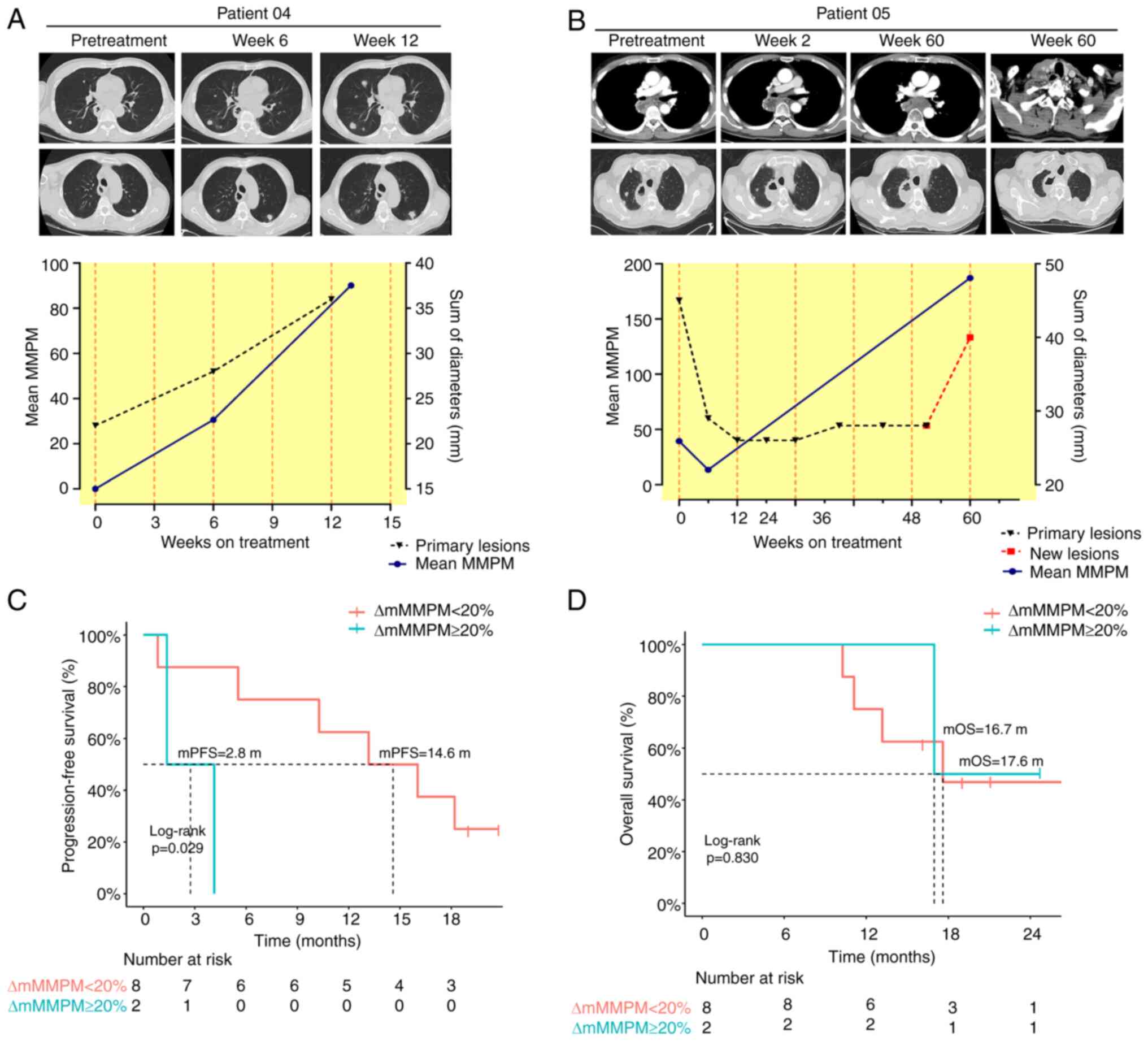
The last pattern, among the patients with ∆mMMPM <20% (n=8), showed a marked reduction or no relatively obvious rise in ctDNA on average at 3 cycles from treatment initiation. All patients showed clinical benefit with at least PR or SD, with a PFS of >6 months, except for one patient who had assessed PD. For instance, for patient 05, ctDNA-based molecular analyses showed a marked reduction in molecular response at cycle 2, which coincided with a radiologic partial response, and at the time of acquired resistance at 60 cycles, while radiographic analysis showed disease progression according to RECIST 1.1(18), consistent with rising ctDNA levels during tislelizumab immunotherapy (Fig. 4B).
Accordingly, ctDNA dynamic changes expressed as the ∆mMMPM more accurately predicted PFS and OS than tTMB (Fig. S1C and D). Patients with ∆mMMPN<20% had significantly longer PFS than patients with ∆mMMPN ≥20% (14.6 vs. 2.8 months; P=0.029) (Fig. 4C), although no significant differences were observed in OS (17.6 vs. 16.7 months; P=0.830) (Fig. 4D). To a certain extent, ∆mMMPN <20% was an independent predictor of PFS in patients receiving second-line tislelizumab monotherapy for advanced and metastatic ESCC.
Discussion
Anti-PD-1 immunotherapy provides long-term survival benefits for patients with advanced ESCC. However, conventional imaging examinations cannot always reliably predict clinical benefits and survival in response to anti-PD-1/PD-L1 therapy due to tumor immune infiltration. Certain patients lose the opportunity to continue receiving immunotherapy due to pseudoprogression and some patients may develop hyperprogressive disease during immunotherapy (25,26). Discriminating patients who benefit from therapy from those who may progress before imaging examinations is a challenge faced by clinical oncologists. Previous studies have shown that ctDNA dynamic changes can sensitively monitor the efficacy of chemotherapy or targeted therapy in patients at an early stage, and ctDNA can better overcome tumor heterogeneity and represent the change in the tumor burden of patients (12-14).
Multiple clinical studies have confirmed that anti-PD-1 immunotherapy combined with chemotherapy is the standard first-line regimen for ESCC (27-30). Second-line anti-PD1 immunotherapy is superior to conventional chemotherapy in patients with ESCC who have received chemotherapy as first-line therapy (6,7,8,17). The present study found that the mPFS and mOS of patients with ESCC receiving second-line tislelizumab were 7.9 and 17.6 months, respectively. This is a partial result of the RATIONALE-302 trial and it is basically consistent with the published results of the whole RATIONALE-302 study (17). The survival time was higher than that reported in other studies, which may be due to the bias caused by the small sample size in the present study. Due to practical reasons, such as sample quality control and financial circumstances, patients from other centers were not included in the present study. With the current National Medical Products Administration of China approved indication for tislelizumab in second-line monotherapy in ESCC, real-world studies with larger sample sizes may be initiated in the future to obtain more evidence-based results. The present study also found that patients with liver metastasis were significantly less likely to benefit from anti-PD1 immunotherapy than patients without liver metastasis, which was consistent with the results of other studies (30,31), suggesting that subjects with ESCC with liver metastasis are potentially a group of patients who are not sensitive to immune monotherapy.
In the present study, certain high-frequency mutated genes were identified in ESCC, such as TP53 and genes involved in the cell cycle, such as FGF19 and CCND1, which is consistent with previously reported results (32). TSC2, ZFN217 mutation and FGF19 amplification were negative predictors in patients with ESCC who received second-line tislelizumab. However, the mechanism of these two gene variants affecting PD-1/PD-L1 is not clear, which is also the study focus of our future work. The present study also found that patients with ESCC whose ctDNA was not detected during tislelizumab monotherapy had longer PFS and OS than those whose ctDNA was detected.
ctDNA was absent in the plasma during the whole therapy in two patients, and these two patients (patients 11 and 12) did not develop disease progression during >1 year of follow-up, suggesting that patients with ctDNA negativity may benefit from tislelizumab immunotherapy. Changes in mMMPM can predict the benefit of PFS. Patients with ESCC and ∆mMMPN <20% can significantly benefit from tislelizumab monotherapy, although there was no statistically significant change in OS. To our knowledge, this is the first study to systematically evaluate the efficacy and prognostic utility of ctDNA in a cohort of patients with ESCC treated with tislelizumab as a second-line monotherapy. Since the present analysis was exploratory, future studies will be needed to validate our findings, including the ∆mMMPM cutoff point. In addition, it would be interesting to combine ctDNA analysis with other potential clinical or molecular predictors of outcome in multiparameter models that may further improve outcome prediction.
However, the present study had certain limitations. It was a prospective study with a relatively small sample size. Furthermore, owing to the lack of tumor tissue after immunotherapy, the present observation of putative emergent mutations in a subset of patients must be interpreted with caution, given that we cannot be entirely certain that these mutations originate from tumor cells. Future studies investigating emergent mutations should profile metastatic/recurrent tumor deposits in addition to pre- and post-immunotherapy plasma samples to conclusively establish the presence of these mutations in tumor cells.
In conclusion, in an analysis of cfDNA in plasma samples from patients who underwent tislelizumab immunotherapy for ESCC, the detection of ctDNA was associated with anti-tumor effects, progression and disease-specific survival. It was demonstrated that ctDNA sequencing is promising for predicting response and relapse after tislelizumab immunotherapy as a second-line monotherapy for advanced ESCC.
Supplementary Material
Tumor mutation profiles included high-frequency alterations in genes associated with (A) PFS and (B) OS. When tTMB was calculated, patients with tTMB-H had (C) longer PFS and (D) OS than patients with tTMB-L, although no significant differences were observed. mPFS, median progression-free survival; mOS, median overall survival; HR, hazard ratio; tTMB-H, tissue tumor mutation burden high.
Circulating tumor DNA results for all 35 plasma samples collected in this study.
Acknowledgements
The preliminary results of this study were presented as a poster at the 2020 World Congress on Lung Cancer meeting (virtual conference; abstract no. 2443) (33).
Funding
Funding: This work was supported by the Zhejiang Provincial Medical Health Science and Technology Project (grant no. 2022KY631) and the Zhejiang Province TCM Science and Technology Project (grant no. 2021ZB035). The study sponsors had no role in the study design, data collection, analysis, interpretation, writing of the report or the decision to submit the manuscript for publication.
Availability of data and materials
The datasets supporting the conclusions of this study are included within the article and its additional files. All mutations reported in this study are provided in Table SI. The data presented in the study are deposited in the Genome Sequence Archive for Human (GSA-Human) repository (https://bigd.big.ac.cn/gsa-human/; accession no. HRA005982).
Authors' contributions
Conceptualization and design: QH, JY, MW, XY; methodology development: QH, XS, YJ; data acquisition: QH, XS, YJ, CG, XY; data analysis and interpretation (e.g., statistical analysis, bioinformatics and other computational analyses): QH, JY, MW; writing and/or revision of the manuscript: QH, JY, MW; administrative, technical or material support (e.g., reporting or organizing data, constructing databases): QH, XY. QH and XY checked and confirmed the authenticity of the raw data and supervised the study. All authors have read and approved the final manuscript.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Zhejiang Cancer Hospital (Hangzhou, China) and all patients provided written informed consent. The study was conducted in accordance with the established ethical standards of the institutional and/or national research committee, as outlined in the Declaration of Helsinki.
Patient consent for publication
The authors confirm that they have obtained written consent from each patient to publish the manuscript.
Competing interests
JY and MW are employees of Nanjing Geneseeq Technology Inc. The remaining authors have no competing interests to declare.
References
|
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Arnold M, Soerjomataram I, Ferlay J and Forman D: Global incidence of oesophageal cancer by histological subtype in 2012. Gut. 64:381–387. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, Chow LQ, Vokes EE, Felip E, Holgado E, et al: Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 373:1627–1639. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Asaoka Y, Ijichi H and Koike K: PD-1 Blockade in tumors with mismatch-repair deficiency. N Engl J Med. 373(1979)2015.PubMed/NCBI View Article : Google Scholar | |
|
Nghiem PT, Bhatia S, Lipson EJ, Kudchadkar RR, Miller NJ, Annamalai L, Berry S, Chartash EK, Daud A, Fling SP, et al: PD-1 blockade with pembrolizumab in advanced Merkel-cell carcinoma. N Engl J Med. 374:2542–2552. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Kato K, Cho BC, Takahashi M, Okada M, Lin CY, Chin K, Kadowaki S, Ahn MJ, Hamamoto Y, Doki Y, et al: Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 20:1506–1517. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Kojima T, Shah MA, Muro K, Francois E, Adenis A, Hsu CH, Doi T, Moriwaki T, Kim SB, Lee SH, et al: Randomized Phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J Clin Oncol. 38:4138–4148. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Huang J, Xu J, Chen Y, Zhuang W, Zhang Y, Chen Z, Chen J, Zhang H, Niu Z, Fan Q, et al: Camrelizumab versus investigator's choice of chemotherapy as second-line therapy for advanced or metastatic oesophageal squamous cell carcinoma (ESCORT): A multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 21:832–842. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Schneider PRM, Metzger R, Schaefer H, Baumgarten F, Vallbohmer D, Brabender J, Wolfgarten E, Bollschweiler E, Baldus SE, Dienes HP and Hoelscher AH: Response evaluation by endoscopy, rebiopsy, and endoscopic ultrasound does not accurately predict histopathologic regression after neoadjuvant chemoradiation for esophageal cancer. Ann Surg. 248:902–908. 2008.PubMed/NCBI View Article : Google Scholar | |
|
Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, Schadendorf D, Dummer R, Smylie M, Rutkowski P, et al: Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 373:23–34. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Bidard FC, Weigelt B and Reis-Filho JS: Going with the flow: From circulating tumor cells to DNA. Sci Transl Med. 5(207ps14)2013.PubMed/NCBI View Article : Google Scholar | |
|
Diaz LA Jr and Bardelli A: Liquid biopsies: Genotyping circulating tumor DNA. J Clin Oncol. 32:579–586. 2014.PubMed/NCBI View Article : Google Scholar | |
|
Alix-Panabières C and Pantel K: Clinical applications of circulating tumor cells and circulating tumor DNA as liquid biopsy. Cancer Discov. 6:479–491. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, Thornton K, Agrawal N, Sokoll L, Szabo SA, et al: Circulating mutant DNA to assess tumor dynamics. Nat Med. 14:985–990. 2008.PubMed/NCBI View Article : Google Scholar | |
|
Lu J, Zhong H, Wu J, Chu T, Zhang L, Li H, Wang Q, Li R, Zhao Y, Gu A, et al: Circulating DNA-Based sequencing guided anlotinib therapy in non-small cell lung cancer. Adv Sci (Weinh). 6(1900721)2019.PubMed/NCBI View Article : Google Scholar | |
|
Siravegna G, Mussolin B, Buscarino M, Corti G, Cassingena A, Crisafulli G, Ponzetti A, Cremolini C, Amatu A, Lauricella C, et al: Clonal evolution and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat Med. 21:795–801. 2015.PubMed/NCBI View Article : Google Scholar | |
|
Shen L, Kato K, Kim SB, Ajani JA, Zhao K, He Z, Yu X, Shu Y, Luo Q, Wang J, et al: Tislelizumab versus chemotherapy as second-line treatment for advanced or metastatic esophageal squamous cell carcinoma (RATIONALE-302): A Randomized Phase III Study. J Clin Oncol. 40:3065–3076. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Schwartz LH, Seymour L, Litière S, Ford R, Gwyther S, Mandrekar S, Shankar L, Bogaerts J, Chen A, Dancey J, et al: RECIST 1.1-Standardisation and disease-specific adaptations: Perspectives from the RECIST Working Group. Eur J Cancer. 62:138–145. 2016.PubMed/NCBI View Article : Google Scholar | |
|
Bosman FT, Carneiro F, Hruban RH and Theise ND: WHO classification of tumours of 485 the Digestive System, 4th edition. Lyon, IARC, Chapter 2, pp15-37, 2010. | |
|
Yang Z, Yang N, Ou Q, Xiang Y, Jiang T, Wu X, Bao H, Tong X, Wang X, Shao YW, et al: Investigating novel resistance mechanisms to Third-Generation EGFR tyrosine kinase inhibitor osimertinib in non-small cell lung cancer patients. Clin Cancer Res. 24:3097–3107. 2018.PubMed/NCBI View Article : Google Scholar | |
|
Fang W, Ma Y, Yin JC, Hong S, Zhou H, Wang A, Wang F, Bao H, Wu X, Yang Y, et al: Comprehensive genomic profiling identifies novel genetic predictors of response to Anti-PD-(L)1 therapies in non-small cell lung cancer. Clin Cancer Res. 25:5015–5026. 2019.PubMed/NCBI View Article : Google Scholar | |
|
Max MX, Bendell JC, Hurwitz HI, Ju C, Lee JJ, Lovejoy A, Mancao C, Nicholas A, Price R, Sommer N, et al: Disease monitoring using Post-induction circulating tumor DNA analysis following First-Line therapy in patients with metastatic colorectal cancer. Clin Cancer Res. 26:4010–4017. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Herrera AF, Tracy S, Croft B, Opat S, Ray J, Lovejoy AF, Musick L, Paulson JN, Sehn LH and Jiang Y: Risk profiling of patients with relapsed/refractory diffuse large B-cell lymphoma by measuring circulating tumor DNA. Blood Adv. 6:1651–1660. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET and Carbone PP: Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 5:649–655. 1982.PubMed/NCBI | |
|
Xu J, Li Y, Fan Q, Shu Y, Yang L, Cui T, Gu K, Tao M, Wang X, Cui C, et al: Clinical and biomarker analyses of sintilimab versus chemotherapy as second-line therapy for advanced or metastatic esophageal squamous cell carcinoma: A randomized, open-label phase 2 study (ORIENT-2). Nat Commun. 13(857)2022.PubMed/NCBI View Article : Google Scholar | |
|
Zhou YX, Chen P, Sun YT, Zhang B and Qiu MZ: Comparison of PD-1 inhibitors in patients with advanced esophageal squamous cell carcinoma in the Second-Line setting. Front Oncol. 11(698732)2021.PubMed/NCBI View Article : Google Scholar | |
|
Luo H, Lu J, Bai Y, Mao T, Wang J, Fan Q, Zhang Y, Zhao K, Chen Z, Gao S, et al: Effect of camrelizumab vs placebo added to chemotherapy on survival and progression-free survival in patients with advanced or metastatic esophageal squamous cell carcinoma: The ESCORT-1st randomized clinical trial. JAMA. 326:916–925. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Doki Y, Ajani JA, Kato K, Xu J, Wyrwicz L, Motoyama S, Ogata T, Kawakami H, Hsu CH, Adenis A, et al: Nivolumab combination therapy in advanced esophageal Squamous-Cell carcinoma. N Engl J Med. 386:449–462. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Wang ZX, Cui C, Yao J, Zhang Y, Li M, Feng J, Yang S, Fan Y, Shi J, Zhang X, et al: Toripalimab plus chemotherapy in treatment-naive, advanced esophageal squamous cell carcinoma (JUPITER-06): A multi-center phase 3 trial. Cancer Cell. 40:277–288.e3. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Sun JM, Shen L, Shah MA, Enzinger P, Adenis A, Doi T, Kojima T, Metges JP, Li Z, Kim SB, et al: Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): A randomised, placebo-controlled, phase 3 study. Lancet. 398:759–771. 2021.PubMed/NCBI View Article : Google Scholar | |
|
Thuss-Patience P and Stein A: Immunotherapy in squamous cell cancer of the esophagus. Curr Oncol. 29:2461–2471. 2022.PubMed/NCBI View Article : Google Scholar | |
|
Chen G, Zhu YJ, Chen J, Miao F, Wu N, Song Y, Mao BB, Wang SZ, Xu F and Chen ZM: Mutational landscape of DNA damage response deficiency-related genes and its association with immune biomarkers in esophageal squamous cell carcinoma. Neoplasma. 69:1314–1321. 2022.PubMed/NCBI View Article : Google Scholar | |
|
He Q and Yu X: P14.15 Circulating Tumor DNA Predict the response and survival after tislelizumab immunotherapy for advanced esophageal squamous cell carcinoma. J Thoracic Oncol. 16 (Suppl)(S336)2021. |









